சுகாதார ஊழியர்களை பரிசோதிக்கத்தவறும் இந்தியா; அவர்களுக்கும் நோயாளிகளையும் ஆபத்து

ஜெய்ப்பூர்: மும்பையின் கிங் எட்வர்ட் மெமோரியல் (KEM - கேஇஎம்) மருத்துவமனை செவிலியர் ரஷ்மிக்கு (பெயர் மாற்றப்பட்டுள்ளது), மே 21இல் நடந்த பரிசோதனையில் கோவிட்-19 உறுதி செய்யப்பட்டது. இந்தியாவின் சோதனை வழிகாட்டுதலின் கீழ், இவ்வாறு பரிசோதனை நடத்துவதற்காக எந்தவொரு அறிகுறியும் அவருக்கு இல்லை. ஆனால் ஐந்து நாட்களுக்கு முன்புதான், தொற்று நேர்மறை உறுதி செய்யப்பட்ட சக ஊழியர் ஒருவருடன் அவர் தொடர்பில் இருந்துள்ளார்.
மே 20 அன்று தனது மாதிரிகள் சேகரிக்கப்படுவதற்கு முன்பு வரை, ரஷ்மி ஐந்து நாட்கள் தொடர்ந்து பணியாற்றினார். "சில செவிலியர்கள் உடனடியாக தனிமைப்படுத்தப்பட்டனர்; ஆனால் மருத்துவமனைகளில் ஊழியர் பற்றாக்குறை இருப்பதால் அனைவருமே அவ்வாறு இல்லை," என்று, இந்தியா ஸ்பெண்டிடம் அவர் தெரிவித்தார். கடைசியில் மே 21 அன்று, அவரும் தனிமைப்படுத்தப்பட்டார்.
கோவிட்-19 ஐ ஏற்படுத்தும் சார்ஸ்-கோவிட்-2 என்ற வைரஸால் சுகாதாரப் பணியாளர்கள் அதிகம் பாதிக்கப்படுகின்றனர்; ஆனால் கோவிட்-19 மருத்துவமனைகள், தனிமைப்படுத்துவதற்கான மையங்கள் அல்லது கோவிட் அல்லாத மருத்துவ மையங்களில் பணிபுரியும் மருத்துவர்கள், செவிலியர்கள் மற்றும் உதவி ஊழியர்கள் உட்பட அதன் சுகாதாரப்பணியாளர்களை தவறாமல் பரிசோதிப்பது தொடர்பாக இந்தியாவிடம் எந்த கொள்கையும் கிடையாது. சுகாதாரப் பணியாளர்களுக்காக இத்தகைய சோதனைகளில் பற்றாக்குறை நிலவுவது, அவர்களையும் அவர்களின் சகாக்கள், நோயாளிகள் மற்றும் சமூகத்தை அதிக ஆபத்தில் ஆழ்த்தும் என்பதை ஆய்வு காட்டுகிறது.
இவ்வாறு இருந்தபோதும், இந்திய சுகாதார மற்றும் குடும்பநல அமைச்சகம் (MOHFW) மே 15 அன்று வெளியிட்ட அறிவிப்பில், தவறாக கோவிட்-19 என வெளிப்படுத்தி இருந்தாலோ அல்லது தனிப்பட்ட பாதுகாப்பு உபகரணங்கள் (PPE) இல்லாத காரணத்தினாலோ சுகாதார ஊழியர்களை தனிமைப்படுத்த வேண்டிய அவசியமில்லை என்று கூறியிருந்தது. ஜூன் 19 அன்று, செவிலியர் சங்கம் ஒன்று உச்சநீதிமன்றத்தில் தாக்கல் செய்த மனுவுக்கு பதிலளித்த மத்திய அரசு, கோவிட்-19 பணியில் உள்ள செவிலியர்கள் அனைவரும் கட்டாயம் ஏழு நாள் தனிமைப்படுத்த வேண்டும் என்று மாநில அரசுகளுக்கு உத்தரவிட்டு உள்ளதாக, செவிலியர் சங்க வழக்கறிஞர் இந்தியா ஸ்பெண்டிடம் கூறினார்.
ஆரம்பத்தில், பல மருத்துவமனைகள் தங்கள் தொழிலாளர்களை கோவிட்-19 வார்டுகளில், 14 முதல் 15 நாள் வரை இரண்டு சுழற்சிகளாய் தனிமைப்படுத்தலுக்கு அனுப்பின. ஆனால் நோயாளிகளின் எண்ணிக்கை அதிகரித்த போது ஊழியர்களின் பற்றாக்குறை ஏற்பட்டது; இதனால், நகர மையங்களில், குறிப்பாக டெல்லி மற்றும் மும்பை போன்ற இடங்களில் செவிலியர் தனிமைப்படுத்தப்பட்ட காலம் மூன்று நாட்கள் என்று சுருக்கப்பட்டதாக, செவிலியர் சங்கங்கள் இந்தியா ஸ்பெண்டிடம் தெரிவித்தன. சுகாதாரம் மற்றும் சுகாதார ஊழியர்கள் விஷயத்தில் மாநிலங்களே சுயமாக விதிகளை உருவாக்குகின்றன, சில நேரங்களில் மத்திய அரசின் வழிகாட்டுதலின் அடிப்படையில் ஏற்படுத்தப்படுகிறது. கோவிட்-19 இன் உயர் விகிதங்களை கொண்ட பெரும்பாலான மாநிலங்களில், சுகாதாரப் பணியாளர்களை தனிமைப்படுத்துவது அல்லது பரிசோதிப்பது குறித்த விதிகளை பின்பற்றுவதில் தீவிரம் காட்டுவதில்லை என்று தொழிற்சங்கங்கள் தெரிவித்துள்ளன.
"இந்த [மத்திய அரசின்] வழிகாட்டுதல்களை நடைமுறைப்படுத்துவது மாநிலத்திற்கு மாநிலம் மற்றும் மருத்துவமனைக்கு மருத்துவமனைக்கு மாறுபடுகிறது," என்று சுயாதீன ஆராய்ச்சியாளரும், சுகாதாரப் பணியாளர்களுக்கு பயிற்சி அளிக்கும் அமைப்பான சேவா சக்தி நிறுவனருமான சுவாதி ராணி கூறினார். கோவிட்-19 கவனிப்புக்காக எந்த நகரம் மற்றும் எந்த மருத்துவமனையில் பணிபுரிகிறார்கள் அல்லது அனுமதிக்கப்படுகிறார்கள் என்பதன் அடிப்படையில் செவிலியர்களின் அனுபவங்களும் மாறுபடும் என்று செவிலியர் சங்கங்கள் தெரிவித்துள்ளன.
மோசமான ஆதரவு, குறையும் மனஉறுதி
நிச்சயமற்ற தனிமைப்படுத்தப்பட்ட காலம், வழக்கமான சோதனை உத்தி மற்றும் தனிமைப்படுத்தப்பட்ட பகுதியில் உரிய வசதி இல்லாதது போன்றவற்றால், சுகாதார ஊழியர்கள் தங்கள் குடும்பங்களில் அதை காட்டிக் கொள்வதில்லை; அக்குடும்பங்கள் பெரும்பாலும் சிறிய வீடுகளில் வசிக்கும்; இதுபோன்ற சூழலால் மன உறுதி குறைவதோடு, அமைப்பின் மீதான நம்பிக்கையும் இழப்பதாக, செவிலியர்கள் தெரிவித்தனர். "அனைத்து ஊழியர்களும் விரக்தியடைந்துள்ளனர்" என்று யுனைடெட் செவிலியர் சங்கத்தின் ஜோல்டின் பிரான்சிஸ் கூறினார்.
“வென்டிலேட்டர்கள் அல்லது வார்டுகளை போல் சுகாதார ஊழியர்கள் அவசரமாக உற்பத்தி செய்யவோ அல்லது 100% பயன்படுத்தி நீண்ட காலத்திற்கு இயக்கவோ முடியாதவர்கள். அரசுகள் அவர்களை வெறுமனே பணியமர்த்துவதை மட்டுமே பார்க்க வேண்டியது அவசியம், ஆனால் மனிதர்களாக பார்க்க வேண்டும்,”என்று தி லான்செட் என்ற மருத்துவ இதழின் தலையங்கம் குறிப்பிட்டது.
தொற்றுநோய் தொடங்கியதில் இருந்து, இந்தியாவின் சுகாதாரப்பணியாளர்களுக்கு தனிப்பட்ட பாதுகாப்பு உபகரணங்கள் பற்றாக்குறை, தாமதமான சம்பள பட்டுவாடா, அடிக்கடி மாறும் தனிமைப்படுத்துதலுக்கான விதிகள், தனிமைப்படுத்தப்படுத்துவதற்கு வசதி இல்லாமை, நீண்ட வேலைநேரம் மற்றும் தங்களது பாதுகாப்பை புறக்கணிப்பது ஆகியவற்றை எதிர்ப்பதாக, செவிலியர் சங்கங்கள் இந்தியா ஸ்பெண்டிடம் தெரிவித்தன."சுகாதாரத்தொழில் கலாச்சாரம் என்பது, ஊழியர்களை சார்ந்ததாக இல்லை; ஊழியர்களின் ஆரோக்கியத்திற்கு முன்னுரிமை கிடையாது" என்று சேவாசக்தி அமைப்பின் ராணி கூறினார்.
ஜூன் 14 அன்று, யுனைடெட் செவிலியர் சங்கத்தால் பிரதிநிதித்துவப்படுத்தப்பட்ட சுகாதாரப்பணியாளர்கள், கோவிட்-19 வார்டுகளில் பணிபுரியும் அனைவருக்கும் அல்லது கோவிட்-19 சந்தேகத்திற்குரியவர்களுடன் பணிபுரியும் போது தனிப்பட்ட பாதுகாப்பு உபகரணங்கள் தேவையென்று கேட்டனர். கோவிட் வார்டுகளில் பணிபுரிபவர்களுக்கு தங்குமிடம் மற்றும் அவர்களுக்கு வேலைக்குச் செல்ல சத்தான உணவு மற்றும் போக்குவரத்து வசதிகள் தேவையெனவும், இறந்த உடல்களின் கண்ணியமாக நடத்துதல் தொடர்பாகவும் உச்ச நீதிமன்றத்தில் தொடரப்பட்ட வழக்கில், குறுக்கீடு மனு மூலம் இந்த கோரிக்கை விடுக்கப்பட்டுள்ளது.
மருத்துவமனைகள் அனைத்து நோயாளிகளையும் பரிசோதிக்க வேண்டும் மற்றும் சந்தேகத்திற்குரிய நோயாளிகளை தாமதமின்றி சோதிக்க வேண்டும்; தொற்று கட்டுப்பாடு மற்றும் தனிப்பட்ட பாதுகாப்பு உபகரணங்கள் அகற்றுவது குறித்து சுகாதாரப் பணியாளர்களுக்கு பயிற்சியளிக்கவும், பணியாளர்களுக்கு தனித்தனி, சுகாதாரமான கழிவறைகளை வழங்கவும், பணியில் இருக்கும்போது தொற்றுநோய்களுக்கு இலவச சோதனை மற்றும் சிகிச்சையையும் வழங்க வேண்டும் என்று அவர்கள் கோரினர். அவர்கள் சரியான நேரத்தில் மற்றும் முழு சம்பளம் தரப்பட வேண்டும்; சுகாதார ஊழியருக்கு பணிபுரியும் காலத்தில் கோவிட் தொற்று ஏற்பட்டால், சம்பளத்தில் குறைப்பு செய்யக்கூடாது எனவும், அவர்கள் வலியுறுத்தினர்.இந்த மனுவுக்கு பதிலளித்த மத்திய அரசு தனது மனுவில், கோவிட்-19 பணியில் இருப்பவர்களுக்கு ஏழுநாள் தனிமைப்படுத்தலை கட்டாயமாக அமல்படுத்துமாறு அனைத்து மாநில அரசுகளையும் கேட்டுக் கொண்டதாகவும், சுகாதாரப்பணியாளர்களுக்கு சம்பளம் வழங்காதது கிரிமினல் குற்றமாகும் என்ற ஆணையை நிறைவேற்றியுள்ளதாகவும் தெரிவித்தது. இதை, தொழிற்சங்கத்தை சேர்ந்த வழக்கறிஞர் ஒருவர் இந்தியா ஸ்பெண்டிடம் தெரிவித்தார்.
சுகாதாரப்பணியாளர் பரிசோதனை ஏன் முக்கியமானது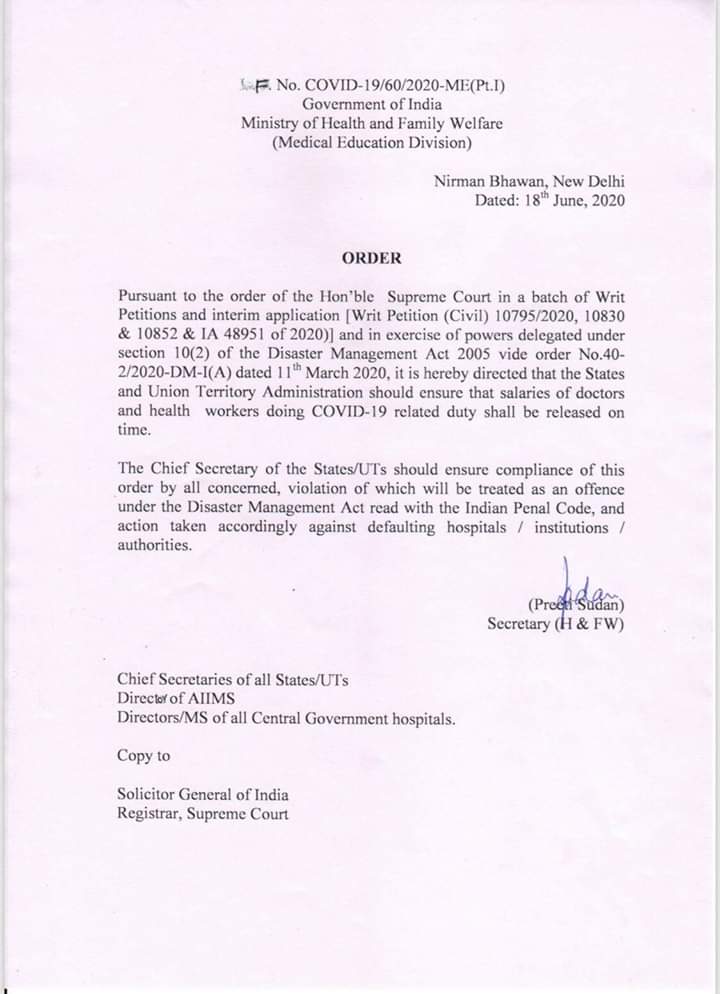{kind=link}
அகில இந்திய மருத்துவ அறிவியல் கழகத்தில் 190-க்கும் மேற்பட்ட சுகாதாரப்பணியாளர்களுடன் சேர்த்து, இந்தியா முழுவதும் பல மாநிலங்களில் சுகாதார மையங்கள் உள்ள நிலையில் தான், கோவிட்-19 தொற்று பரவியது. மும்பையில் மட்டும், பிரஹன்மும்பை முனிசிபல் கார்ப்பரேஷன் மருத்துவமனைகளில் 5,000 செவிலியர்களில் 4% பேர் சுகாதார மையம் அல்லது சமூக அளவில், கோவிட் -19ஆல் பாதிக்கப்பட்டு உள்ளதாக, பிரஹன்மும்பை முனிசிபல் கார்ப்பரேஷன் நர்சிங் மற்றும் பாரா மெடிக்கல் ஸ்டாப் யூனியனின் ரஞ்சனா அத்வாலே தெரிவித்தார். "இந்த வழக்குகள் பல கோவிட் அல்லாத வார்டுகள் மற்றும் மருத்துவமனைகளில் இருந்து வருகின்றன; ஆனால் நகர அளவிலான அல்லது நாடு முழுவதுமான எண்ணிக்கை கிடைக்கவில்லை" என்று ராணி மேலும் கூறினார்.இந்த அனுபவங்கள் சார்ஸ்-கோவ்-2 ஆல் சுகாதாரப் பணியாளர்கள் அளவுக்கு அதிகமாக பாதிக்கப்பட்டுள்ள பிற நாடுகளுடன் ஒத்துப்போகின்றன. ஏப்ரல் 23 வரை சீனாவிலும் ஐரோப்பாவிலும் (சீனா 3.8%, ஜெர்மனி 4.6%, இத்தாலி 9% மற்றும் ஸ்பெயினில் 19%) கோவிட்-19 வழக்குகளில் 4% முதல் 19% வரை அவை உள்ளதாக, இம்பீரியல் கல்லூரியின் கோவிட்-19 மறுமொழி குழுவின் அறிக்கை தெரிவிக்கிறது.
சுகாதாரப் பணியாளர்கள் மீது வாராந்திர ஆர்டி-பி.சி.ஆர் சோதனைகளை நிர்வகிப்பது மற்றும் முடிவுகள் 24 மணி நேரத்திற்குள் கிடைப்பதை உறுதி செய்வது அறிகுறிகளின் அடிப்படையில் சுய தனிமைப்படுத்தப்படுவதை விட கோவிட்-19 பரவுதலை 16-23% குறைக்கும் என்று கல்வி ஆராய்ச்சி மேற்கோளிட்டு அறிக்கை குறிப்பிட்டது.மேலும், முந்தைய தொற்றுநோய்களில், சுகாதாரப்பணியாளர்களுக்கான கண்காணிப்பு திட்டங்கள் “மன உறுதியை அதிகரித்தன; வருகை குறைந்துவிட்டன மற்றும் நீண்டகால உளவியல் தாக்கங்களைக் குறைக்கக்கூடும்”, என்று, இங்கிலாந்தில் உள்ள ஒரு தேசிய சுகாதார அமைப்பு மருத்துவமனையில் சுகாதாரப்பணியாளர்களுக்கான கோவிட் -19 குறித்த ஆய்வின் ஆசிரியர்கள் எழுதினர். பாதிக்கப்படக்கூடிய நோயாளிகளை ஒரு தொற்று பணியாளர்கள் மற்றும் சுகாதார ஊழியர்களில் கோவிட்-19 பரவலில் இருந்து இத்தகைய கண்காணிப்பு பாதுகாக்கிறது, அதேநேரத்தில் நோயாளியின் நம்பிக்கையையும் சுகாதார சேவைகளை அணுகுவதற்கான விருப்பத்தையும் அதிகரிக்கிறது.
"வழக்கமான சோதனைகள் நமது சுகாதார ஊழியர்களின் நம்பிக்கை அளவை மேம்படுத்தும்" என்று யுனைடெட் செவிலியர் சங்கத்தின் பிரான்சிஸ் கூறினார்.ஆனால் இந்தியாவில் உள்ள கோவிட்-19 மருத்துவமனைகளில் சுகாதாரப் பணியாளர்களை தொடர்ந்து தனிமைப்படுத்துவது அல்லது பரிசோதிப்பது குறித்து எந்த வழிகாட்டுதல்களும் இல்லை என்று செவிலியர்கள் மற்றும் பொது சுகாதார நிபுணர்கள், இந்தியா ஸ்பெண்டிடம் தெரிவித்தனர்.
இந்தியாவும், சுகாதாரப்பணியாளர் கண்காணிப்பும்
பாதுகாப்பு உபகரணங்கள் இல்லாமல் கோவிட்-19 வெளிப்பட்டு வரும் சூழலில், சுகாதாரப்பணியாளர்களுக்கான தனி கோவிட் 19 பரிசோதனை வழிகாட்டுதல்கள் இந்தியாவில் இல்லை. மே 18 அன்று அறிவிக்கப்பட்ட சமீபத்திய தனது கோவிட்-19 சோதனை உத்தியில் இந்திய மருத்துவ ஆராய்ச்சி கவுன்சில், கோவிட்-19ஐ கட்டுப்படுத்துதல் அல்லது தணித்தல் மற்றும் இன்ஃப்ளூயன்ஸா போன்ற நோய்களின் அறிகுறிகளைக் கொண்ட (காய்ச்சல் ≥ 38 ° C மற்றும் இருமலுடன் கடுமையான சுவாசத்தொற்று) முன்வரிசை தொழிலாளர்கள் மட்டுமே சோதிக்கப்படலாம். கோவிட்-19 நோயாளிகளின் நேரடி மற்றும் அதிக ஆபத்து தொடர்புகளால் உறுதிப்படுத்தப்பட்ட வழக்கிற்கு ஆளானவர், ஐந்தாம் மற்றும் பத்தாம் நாளுக்கு இடையில் ஒருமுறை சோதிக்கப்படலாம் என்றது. மேலும், ஹைட்ராக்ஸி குளோரோகுயின், மன அழுத்த மேலாண்மை நடைமுறைகள், பாதுகாப்பு உபகரணங்கள் மற்றும் தொற்று தடுப்பு கட்டுப்பாட்டில் பயிற்சி ஆகியவற்றை சுகாதார மற்றும் குடும்ப நல அமைச்சகம் பரிந்துரைக்கிறது. உறுதிப்படுத்தப்பட்ட கோவிட்-19 தொற்றுக்கு ஆளான அனைத்து சுகாதாரப் பணியாளர்கள் மற்றும் உதவியாளர்கள் தனிமைப்படுத்தப்பட்டு 14 நாட்களுக்கு பிறகே பணியை தொடரப்பட வேண்டும் என்று அவர்களின் வழிகாட்டுதல்கள் குறிப்பிடுகின்றன. கூடுதலாக, அவை ஏழு வாரங்களுக்கு ஹைட்ராக்ஸி குளோரோகுயின் (HCQ) உட்கொள்ள வேண்டும். (கோவிட்-19க்கான தடுப்பு மருந்தாக ஹைட்ராக்ஸி குளோரோகுயினை எவ்வாறு பயன்படுத்துவது என்பது பற்றிய சிறிய ஆதாரங்களின் அடிப்படையில் எங்கள் கட்டுரையை படியுங்கள்).
ஒரு கோவிட் வார்டில் 14 நாள் இருந்து முடித்த பிறகும் அல்லது கோவிட் 19இல் இருந்து மீண்ட பிறகும் கூட, அனைத்து செவிலியர்களும் வேலைக்கு அல்லது வீட்டிற்கு திரும்புவதற்கு முன்பு சோதனை செய்யப்பட மாட்டார்கள். கோவிட்-19 மருத்துவ வசதியில் சுமார் 16 நாட்கள் சிகிச்சைக்குப்பிறகு, சுமார் 12 நாள் வீட்டு தனிமைப்படுத்தலுக்காக வீடு திரும்புமாறு ரஷ்மி கேட்டுக் கொள்ளப்பட்டார். “நான் அவர்களிடம் கேட்ட பிறகும் [கோவிட்-19 எதிர்மறையா என்பதை கண்டுபிடிக்க] நான் அவர்கள் எனக்கு இரண்டாவது சோதனையை செய்யவில்லை. எனக்கு வீட்டில் இரண்டு இளம் குழந்தைகள் உள்ளனர். ஆனால் அந்த மையத்தில் அறிகுறியற்ற நோயாளிகளுக்கு இரண்டாவது முறையாக பரிசோதிக்கும் கொள்கை அவர்களிடம் இல்லை என்று கூறினர்,”என்று அவர் கூறினார்.
அறிகுறிகள் தோன்றிய 10 நாட்களுக்கு பிறகு, லேசான மற்றும் மிதமான நோய்வாய்ப்பட்ட நோயாளிகளை மருத்துவமனையில் இருந்து வெளியேற்ற அனுமதிக்கும் வகையில், சுகாதார அமைச்சகம் தனது கொள்கையை திருத்தியது; காய்ச்சல் இல்லாவிட்டால் மற்றும் மூன்று நாட்களுக்கு ஆக்ஸிஜன் சிகிச்சை தேவையில்லை எனில், அதற்கு முன் சோதனை செய்யாமல் வெளியேற்றம் செய்யலாம். நோயாளிகள் அதன்பிறகு ஏழு நாட்கள் வீட்டில் தங்களை தனிமைப்படுத்திக் கொள்ள வேண்டும்.
இதற்கிடையில், கோவிட்-19க்கு எதிரான இந்தியாவின் போராட்டத்தில், சேவையில் ஈடுபடக்கூடிய 2,21,200 சுகாதார ஊழியர்களுக்கு ரூ.50 லட்சம் காப்பீட்டுத்தொகையையும் அரசு அறிவித்துள்ளது.
அறிகுறியற்ற சுகாதார ஊழியர்களை பரிசோதித்தல்
அறிகுறியற்ற மற்றும் அறிகுறியுள்ள சுகாதாரத் தொழிலாளர்கள் தரமான தனிப்பட்ட பாதுகாப்பு உபகரணங்கள் இல்லாத வேலை இடங்களுக்கு தொடர்ந்து செல்வதால், அவர்களை தவறாமல் சோதிக்காமல் இருப்பது ஆபத்தானது என்று லண்டனில் உள்ள புற்றுநோய் பரிணாமம் மற்றும் மரபணு உறுதியற்ற ஆய்வகத்தின் ஆசிரியர்கள் எழுதிய 'The case for health-care worker screening to prevent hospital transmission' என்ற, தி லான்செட் இதழில் வெளியான கட்டுரை தெரிவிக்கிறது. இந்த தொழிலாளர்கள் மருத்துவமனைகளுக்கு உள்ளேயும் வெளியேயும் மற்றவர்களுக்கு இந்த நோயை பரப்பலாம். ஊரடங்கின் போது கூட, மருத்துவமனை ஊழியர்களுக்கு இடையே அறிகுறியற்ற கோவிட்-19 “தொடர்ந்து பரவுவதற்கான ஒரு சக்திவாய்ந்த ஆதாரமாக செயல்படக்கூடும்” என்று கட்டுரை மேலும் கூறியுள்ளது.
இந்தியாவில், பல மருத்துவமனைகளில் வசதிகள் போதுமானதாக இல்லை. பெரும்பாலும், சுகாதாரப் பணியாளர்களுக்கு தனிப்பட்ட பாதுகாப்பு உபகரணங்கள் அணிய, மாற்றுவதர்கு அறை வசதி கூட இல்லை; அவர்களுக்கு என்.95 முகக்கவசங்கள் வழங்கப்படுவதில்லை; இதனால், அவர்கள் வைரஸ் தொற்றால் பாதிக்கப்படுவதாக, கோவிட்-19 வார்டுகளை சேர்ந்த செவிலியர்கள் மற்றும் மருத்துவர்கள், இந்தியா ஸ்பெண்டிடம் தெரிவித்தனர். மகாராஷ்டிராவில் உள்ள ஒரு அரசு மருத்துவமனையில் பணிபுரியும் மருத்துவர் ஒருவர், “நாங்கள் என்.95 முகக்கவசங்களுக்கு பொருத்தமாக சோதனை செய்யும் ஊழியர்கள் அல்ல; தொற்றுநோய்க்கான அபாயத்தை அதிகரிக்கிறோம்” என்றார்.
"நாங்கள் தனிப்பட்ட பாதுகாப்பு உபகரணம் அணியும் அறையை அடைய, கோவிட் வார்டு வழியாகத்தான் செல்ல வேண்டும்" என்று கோவிட் நேர்மறை உறுதி செய்யப்பட்ட செவிலியர் ரஷ்மி கூறினார். "அவசரகால வார்டில், எங்கள் தனிப்பட்ட பாதுகாப்பு உபகரணம் அணியும் அறையானது, நோயாளிகளின் குளியலறைக்கு அருகில் உள்ளது" என்று ரஷ்மி மேலும் கூறினார்.
இத்தகைய அடிப்படைகளின் பற்றாக்குறை, சுகாதாரப் பணியாளர்களைத் தவறாமல் பரிசோதிப்பது மற்றும் கண்காணிப்பது இன்னும் முக்கியமானது என்று உணர்த்துகிறது, ஏனெனில், பலர் அறிகுறியற்றவர்களாக இருக்கலாம்.
The South Korean city of Daegu (population 2.4 million) had the first large outbreak of COVID-19 outside of China. Despite facing similar challenges as other large cities--shortages of personal protective equipment, in-patient beds and healthcare workers--the rate of COVID-19 infections among healthcare workers in Daegu remained lower than in other cities.
A month into the epidemic, 121 healthcare workers were COVID-19 positive, including 14 doctors, 56 nurses and 51 nurse aides--1.8% of the 6,620 confirmed cases at the time. This is lower than other countries such as Italy where 9% of all confirmed cases were of healthcare workers. The study found that nurses were more susceptible to catching the virus: 2.4 per 1,000 doctors were infected compared to 5 per 1,000 for nurses and nurse aides.
This is what Daegu did: Closely monitored shift durations to minimise fatigue that could cause errors in basic infection control, such as hand hygiene and PPE donning and doffing. They limited shifts to two weeks for public sector workers and one month for private sector workers, with 40 hours per week.
They followed a policy of aggressive use of PPE, N95 respirators along with eye protection, shoe covers and coveralls at screening clinics and for the care of all suspected or confirmed COVID-19 patients.
Staff working with COVID-19 patients were screened twice a day for symptoms. Each hospital adapted screening protocols for employees. Anybody who reported symptoms was tested, with results provided within hours, and could work only if they tested negative. If there was a potential cluster outbreak, all staff were tested regardless of symptoms.
All healthcare professionals completing their rotation in a COVID-19 facility were tested regardless of symptoms, and asked to self-quarantine if they had had close contact with a patient without proper PPE, if they had traveled internationally, or if they were part of a specific religious group known to have a high incidence of infection. On the 13th day of quarantine after exposure, healthcare workers were tested and could return to work only on Day 15 if they tested negative.
Source: How South Korea Responded to the Covid-19 Outbreak in Daegu
(கேதன், இந்தியா ஸ்பெண்ட் எழுத்தாளர் / ஆசிரியர் ஆவார். இந்தியா ஸ்பெண்ட் பயிற்சியாளர் சுரபி பரத்வாஜ், இக்ட்டுரைக்கு பங்களிப்பு செய்தார்).
உங்களின் கருத்துகளை வரவேற்கிறோம். கருத்துகளைrespond@indiaspend.org. என்ற முகவரிக்கு அனுப்பலாம். மொழி, இலக்கண நடை கருதி அவற்றை திருத்தும் உரிமை எங்களுக்கு உண்டு.