1 Billion Vaccine Doses, But Women, Tribals Lag
Covid-19 vaccination coverage is lowest in India's tribal-dominated districts and areas, our deep dive into district-level data has found. Women are falling behind in even the better-performing states

Benaulim, Goa and Noida, Uttar Pradesh: India has administered 1.07 billion doses of the Covid-19 vaccine, but an IndiaSpend analysis of granular data shows wide disparities across regions, gender and social groups.
India's most vaccinated district, Mahe in Puducherry, has given at least one dose of a Covid-19 vaccine to more than its usual resident population (non-residents such as migrant workers), recording 108% coverage. The least-vaccinated district, Kurung Kumey in Arunachal Pradesh, has covered only 11%. Mahe also leads in terms of fully vaccinated persons, at 87% of its total population. Kamjong in Manipur has fully vaccinated 6%.
Kurung Kumey and Kamjong are emblematic of how India's Scheduled Tribes (ST) are being left behind in the Covid-19 vaccination drive, thus far. A majority of the bottom 50 districts in terms of coverage with at least one dose have sizeable tribal populations; 36 (72%) are rural, tribal majority districts; two in three are in the north-eastern states. There are large disparities in coverage in districts like Palghar in Maharashtra and Sonbhadra in Uttar Pradesh, which have tribal-dominated blocks, compared to coverage in urban, non-tribal districts in these states.
Public health experts flagged longstanding challenges of delivering health services in far-flung tribal areas. They told us that if the government can carry electoral ballot boxes deep into tribal pockets, it must take the Covid-19 vaccination programme into tribal areas as well.
Women too are falling behind in vaccination coverage. Our analysis of 544 districts, which have given one dose to at least 40% of their total population, shows that in nearly half, the vaccination sex ratio is worse than the sex ratio of their population. The three worst-performing such districts are in the National Capital Region--namely Central Delhi, Gurugram and Gautam Buddha Nagar (Noida). Just 62 women received a vaccine dose for every 100 men in these districts. Vaccination will need to be taken to women's doorsteps, public health experts said.
The government needs to do more to generate awareness about the benefits of vaccination, particularly through community-level messaging, they say, and warn against apathy towards vaccination with daily new Covid-19 cases in India at comparatively low levels at present.
On Wednesday, November 3, nearly 300 days into India's Covid-19 vaccination programme, Prime Minister Narendra Modi will hold a review meeting with district magistrates of over 40 districts with less than 50% coverage of the first dose and low coverage of the second dose of a Covid-19 vaccine. The press release from the Prime Minister's office named Jharkhand, Manipur, Nagaland, Arunachal Pradesh, Maharashtra and Meghalaya among states with districts having low vaccination coverage.
Our analysis shows that, among large states, Uttar Pradesh and Bihar are the two worst performers in terms of administering at least one dose of a Covid-19 vaccine to their total population. More than 90% of the districts in both states are lagging the countrywide average. To be sure, the percentages for Maharashtra and Jharkhand, at 71% and 88%, respectively, are also poor.
Imbalances between states and districts within states
India's vaccination programme allows people to be vaccinated anywhere. Migrant destination states like Maharashtra, Delhi, Gujarat and Haryana will thus vaccinate more persons than are ordinarily resident in their states, whereas states like Uttar Pradesh and Bihar which have higher outward migration, will vaccinate fewer. Read more about our methodology here.
There are large disparities between states in terms of administering at least one dose of a Covid-19 vaccine to their total population. At one end of the scale are states like Himachal Pradesh, Sikkim and Goa, which had given one dose to around 75% of their total population by late-October. At the other end are Nagaland (32%), Meghalaya (33%) and Jharkhand (39%). Of the 700 districts, 329 (47%) are yet to give even one vaccine dose to more than half their total population. The countrywide average is 53%.
Outside the North East, the worst performers are Uttar Pradesh and Bihar. Both have given at least one vaccine dose to 43% and 42% of their total population, respectively. A full 69 (92%) of UP's 75 districts lag the national average. The proportion is even worse in Bihar, with 37 of its 38 districts (97%) lagging the national average. Both states have large migrant labour populations which presumably could have been vaccinated in other states. Not all workers have left for urban employment hubs, though, with unemployment remaining high in both urban and rural India as of October 2021, per Centre for Monitoring Indian Economy data. Many migrant workers who lost work due to lockdowns to control the second Covid-19 wave are reportedly still in their villages. An indication that more workers are in villages than usual during the pandemic is the reported exhaustion of the Mahatma Gandhi National Rural Employment Guarantee Act budget in several states, under the pressure of increased demand for job work, with the rural economy struggling under the adverse economic impact of the second Covid-19 wave.
The state-wise averages also hide large disparities between districts. Even better performing states like Uttarakhand have large percentage point differences in coverage between their most-vaccinated and least-vaccinated districts. In Dehradun, coverage is 74%; in Champawat, 48%.
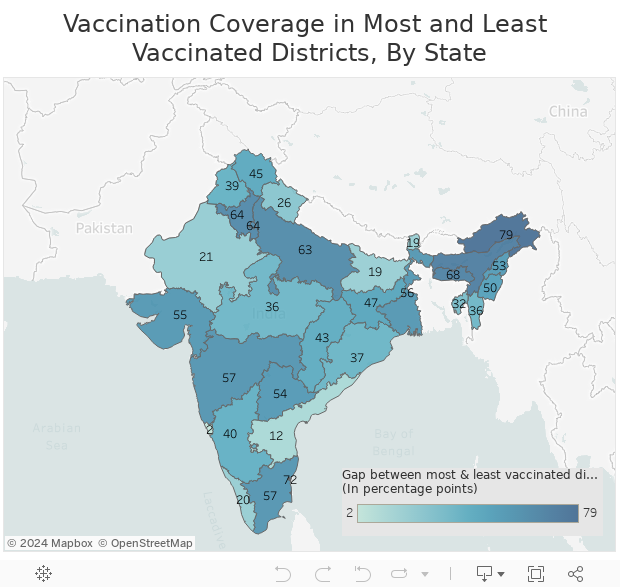
Sources: Covid19India.org, Harvard Dataverse
The gap between most and least vaccinated districts in most states betrays an urban bias in vaccination coverage. The urban-rural gap across India is 10 percentage points. "This gap shows that the focus of India's vaccination programme, and rightly so, was initially in urban areas. With the completion of vaccination in urban and semi-urban areas where the virus was very active, the authorities can now move to the peripheral areas," K. Sujatha Rao, former Union health secretary, told IndiaSpend.
Among the large states, there were, however, more than 10-percentage-point gaps between average vaccinations in urban and rural districts in West Bengal, Haryana, Uttarakhand, Telangana, Punjab and Jharkhand by late October. In Maharashtra and Tamil Nadu, for instance, the most and least vaccinated districts are their capital cities and capital-adjacent districts. There is a 57-percentage-point difference between both Mumbai and neighbouring Palghar district, which has a large Scheduled Tribe population, and between Chennai and neighbouring Thiruvallur district.
Nuh, India's 'most backward' district and the only Muslim-dominated district in Haryana, is another rural district with low coverage that's adjacent to an urban one with high coverage. Nuh was lagging the rest of Haryana in vaccinations, IndiaSpend had reported in April this year. Half a year later, this gap persists, and Nuh is the least vaccinated (40% of the total population) among Haryana's districts, lagging behind the state average of 61% coverage of the total population by 21 percentage points. The gap between Nuh and its neighbouring district Gurugram, one of India's wealthiest, is 64 percentage points.
Karnataka, Andhra Pradesh and Rajasthan have negligible urban-rural gaps in vaccination coverage. Kerala, one of the more urban states, has given more people in rural districts (70%) at least one dose of a Covid-19 vaccine compared to urban districts (65%).
In some northeastern states, the urban-rural divide in people administered at least one dose of a vaccine is even more stark. Among the 11 districts of Nagaland, only Kohima and Dimapur are urban. The gap between these two and the state's nine rural districts is 29 percentage points.
The gap between Manipur's five urban and eight rural districts is 26 percentage points; in Mizoram, 19 percentage points between six urban and two rural districts.
The fourth national serosurvey, conducted in December-January before India's second Covid-19 wave devastated rural India (which had been less affected in the first wave), showed prevalence of antibodies was almost the same in rural (66.7%) and urban areas (69.6%), IndiaSpend reported in July 2021.
"There could be a number of reasons for lower coverage in rural areas: an awareness gap, access gap or an apathy gap," K. Srinath Reddy, president of the Public Health Foundation of India, told IndiaSpend. "Awareness about the immunity provided by two doses of the vaccine may be lacking, as there have been reports of a single dose being sufficient, which is untrue since immunity provided by two doses was also seen to wane after four months in Israel and the UK. Accessibility is an issue that can keep migrant labourers from getting the vaccine. Can they be located and vaccinated wherever they are? Registration on the CoWin portal is another concern for accessibility."
IndiaSpend has asked state governments and district administrations in the north-east, Jharkhand, Chhattisgarh, Punjab, Uttar Pradesh, Bihar and Maharashtra for reasons behind lower vaccination coverage in certain districts and the steps being taken to increase vaccine uptake in these areas. We will update the article when they respond.
Tribal-dominated districts at bottom of vaccinated list
Of 176 tribal districts, 128 (72%) were performing better than the all-India vaccination coverage, the Ministry of Health and Family Welfare had said in June. Our analysis of 192 districts with Scheduled Tribe (ST) population greater than 20% shows that by late October, 121 (63%) were lagging the national average of 53% coverage in terms of persons receiving at least one dose of a Covid-19 vaccine. Moreover, a majority of the bottom 50 districts in terms of coverage with at least one dose have significant ST populations; 36 (72%) are tribal majority districts; 40 are in the northeastern states and Jharkhand.
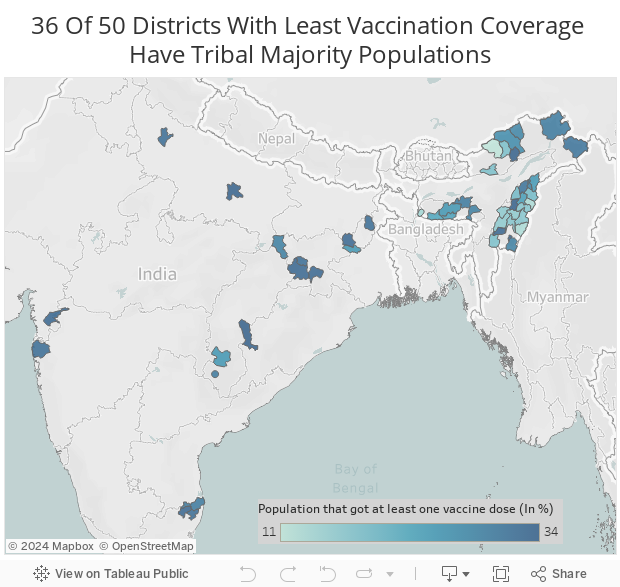
Sources: Census of India, Covid19India.org
Tribal-dominated districts in several states have recorded disproportionately lower vaccine coverage in comparison with other districts, IndiaSpend had reported in June 2021. Indigenous people are more vulnerable than others during the Covid-19 pandemic on account of their higher degree of socio-economic marginalisation, their lack of access to effective monitoring, early-warning systems and health and social services, the United Nations Permanent Forum on Indigenous Issues has said.
"The low coverage in areas and districts with high tribal population is not surprising as logistically the tribal areas are a challenge," said Rao. "Populations are dispersed, the terrain and communications are difficult to negotiate, making access challenging. The public health system presence is typically weak with no doctors. In several pockets, there may be vaccine hesitancy due to lack of right information and concerns of side effects that may affect their ability to work. In addition, shortage of personnel in these areas may be another reason for low coverage."
Union health minister Mansukh Mandaviya had said on October 27 that the central government would undertake door-to-door vaccination. IndiaSpend has asked the ministries for tribal affairs and health and family welfare for reasons for lower vaccination coverage in tribal-dominated areas and for details of steps such as door-to-door vaccination being taken to increase vaccine uptake in these areas. We will update the article when they respond.
National Capital Region has among widest gender gaps in vaccination
Many districts even in the better performing states have recorded wide gender gaps in coverage with at least one dose of a vaccine. In 544 of 700 districts, which have covered at least 40% of their total population, and for which sex ratio data are available, nearly half (46%) have a worse vaccination sex ratio, i.e. number of women vaccinated per 100 men, than the sex ratio of their population. Among the worst performers are districts in the National Capital Region (NCR) and the worst of all is Central Delhi, home to the Indian Parliament. Following Central Delhi at second and third-lowest vaccination sex ratios are Gurguram in Haryana and Gautam Buddha Nagar, UP (Noida), respectively, both in the NCR. An average 62 women have received a vaccine dose for every 100 men in these three districts.
Six of 11 Delhi districts are in the bottom 25, as are other districts in the NCR including Faridabad and Panipat in Haryana. Several of Gujarat's big urban districts Ahmedabad, Surat, Valsad and Bharuch, and Maharashtra's capital, Mumbai, feature in the bottom 25, with 76 women receiving a vaccine dose for every 100 men in these five urban districts, on average.
"The gender gap could be a result of inadequate efforts to reach out to women. They are often invisibilised and special efforts need to be made to reach out to them by getting frontline workers to visit them in their workplaces or homes. They may have concerns and fears of side effects - fever, headache and even death, which is especially worrying for them as homemakers with the responsibility of being the caregivers for their families. These fears need to be explained and the support of the family needs to be obtained. The overall state response has to be motivating and persuasive, not punitive or threatening," said Rao.
"Generally, the health-seeking behaviour of women is poor. Thanks to patriarchy, women's health is not a priority in most households. Travelling a long distance to the vaccination site, particularly if there is no male member to accompany them can prevent them from getting the vaccine," said Reddy.
Way forward for India's vaccination programme
The government will have to take the Covid-19 vaccination programme to remote corners, and address apathy towards vaccination through persuasive and not punitive communication at the community level, public health experts told IndiaSpend.
"Since there is district-level data available with the government, the unique issues in each district can be addressed in a decentralised manner," said Reddy. "The shortfalls in healthcare capacity can be supplemented using mobile teams where needed. To get over accessibility issues in remote areas, vaccines need to be sent as close to the homes if not to the homes directly using mobile vans with cold storage facilities. If we can send ballot boxes there, surely we can send vaccines in cold storage boxes as well."
"We will need to engage with communities and organise community-based vaccination camps," said Rao. "Any resistance must not be met by force or threats but with full disclosure of the risks and benefits of vaccination against Covid-19 and with incentives such as rations to assure people of assistance in case any side effects impact their ability to work on the day following the vaccination."
Reddy concurred. "There is a need to generate awareness about the benefits of the vaccine. Mass media is crucial of course, but community-level messaging is the key. Most people make up their minds about the vaccine based on anecdotes of pain, etc. they gather from their neighbourhood, so involving communities in the communication is important, and something that has been missing so far. The messaging should include the importance of wearing masks and getting both vaccine doses on time to protect against new Covid variants," he said.
To address the gender gap in vaccination in the past, women, who face many cultural barriers while seeking healthcare, were provided with vaccines at their doorstep. "This needs to be replicated," said Reddy.
The government must also guard against apathy toward vaccination at a time when daily new Covid-19 cases are low. "Because there are fewer cases right now, some may have been led to believe that there is no need for them to get a vaccine. This apathy needs to be addressed because new variants of the virus cannot be ruled out," said Reddy.
District population data and claims of 100% vaccination With the decennial census for 2021 delayed due to the Covid-19 pandemic, the latest official district-level population data available are over 10 years old. The district population estimates used here are from the 'Population Estimates for Districts and Parliamentary Constituencies in India, 2020' dataset, published on April 30, 2021 by Harvard University researchers Weiyu Wang, Rockli Kim and S.V. Subramanian. Its population projections for all of India's 736 districts use satellite-based high-resolution settlement mapping (see here and here for more on their methodology of estimation), which, like the Census of India, Unique Identification Authority of India (UIDAI) and India's Covid-19 vaccination program, accounts for the migration of people across state and district borders We analysed districts in all states and two Union territories (Delhi and Puducherry) that have elected governments, and Chandigarh. All told, 700 districts (95%) feature in our analysis. The Harvard data represent total district population, while presently only adults are eligible for vaccination in India. There are no reliable, district-wise adult population estimates for India that are publicly available, since Census 2011, and 2011 data cannot be used due to significant changes in median age projected for different states. Electoral rolls, in which only adults are registered, have been used by some states to claim that they have achieved 100% vaccination of their eligible population. India's electoral roll, however, does not include all adults, and some of these claims are incorrect. "Pratapgarh in Rajasthan was the first district to achieve 100% vaccination, according to the government. The state should be very careful while it makes any such claims as this can lead to slowing down of further vaccination efforts in the district," Chhaya Pachauli, an activist associated with the Prayas Centre for Health Equity in Chittaurgarh and the Jan Swasthya Abhiyan in Rajasthan, told IndiaSpend. "Being a tribal belt, vaccine hesitancy was initially huge in Pratapgarh. Gradually, through consistent efforts of the local administration as well as civil society organisations, the hesitancy has certainly gone down. However, there's still some reluctance and there are still some people left out. This is evident from our own work experience in the area." State assembly constituencies in India also do not account for migration across state and district borders. Lastly, though data used here are estimates of total district populations, the common methodology applied across all districts puts them on an equal footing for analysis. The district-wise sex ratios (females per 100 males in our analysis) and proportion of Scheduled Tribe populations, are taken from Census 2011. Between Census 2011 and October 2021, the reorganisation of districts in several states has seen 96 more districts added to India's total. Not all states have reorganised population data among new and successor districts. Telangana has the best data in this regard; Uttar Pradesh and Tamil Nadu the worst, our analysis showed. Where states have not provided such data, we could not include them for new districts. |
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
