As India Unlocks, Rural Districts Report COVID-19 Surge

Mumbai: On June 1, 2020, 41% of Maharashtra’s COVID-19 cases were outside of Mumbai. As the lockdown has opened and testing has increased, COVID-19 cases in the rest of the state have grown. By September 23, 85.7% of Maharashtra’s cases were outside of Mumbai.
As the fourth phase of opening the lockdown proceeds apace, some districts that currently have few cases of COVID-19 should brace for a surge, experts warn. An analysis of data from the three states with the most active COVID-19 cases shows that almost all of their districts are at risk of a surge, based on test positivity rate and doubling time.
We analysed COVID-19 testing data over six weeks to September 20 for 36 districts across Maharashtra, Karnataka and Andhra Pradesh. Only two districts had the epidemic somewhat under control as seen from their positivity rates and doubling times.
The total lockdown that started March 24 has been lifted in phases -- the first phase of the “unlock” began on June 1. Since then, more and more districts have reported COVID-19 cases. In May, 523 districts were affected by the virus and as of September 20, 636 of 637 districts for which data are available have been affected, with Lakshadweep being the only exception.
“This is like a forest fire; wherever sparks fall the fire will start and then spread. Eventually most towns and villages will be affected, except remote ones with little or no contact with other communities,” T Jacob John, virologist and professor emeritus of Christian Medical College, Vellore, told Indiaspend. “Where case detection and isolation/quarantine is effective, the speed of spread will be slow.”
Across the country, cases have increased nearly 30-fold from 182,143 confirmed cases on May 31, the last day of complete lockdown, to 5.56 million on September 22. It took nearly six months to cross 1 million COVID-19 cases on July 17 and less than two months thereafter to cross the five million-mark on September 16. Currently, India has 975,861 active cases and the highly infectious disease has caused 88,935 deaths, data from the Ministry of Health and Family Welfare (MoHFW) show.
Of the active cases in the country, 57% are from Maharashtra (275,017), Karnataka (95,354), Andhra Pradesh (74,518), Uttar Pradesh (64,164) and Tamil Nadu (46,495), the ministry’s data show. Active infections in other states have also increased, such as Kerala (39,354), Chhattisgarh (37,927) and Odisha (34,033), the next three states with the most COVID-19 cases.
Which districts could become hotspots?
“Any district with a high population density is at equal risk,” Giridhar Babu, head of Life Course Epidemiology at the Public Health Foundation of India, told IndiaSpend. All it takes is a susceptible population and the introduction of infection.
Cities and states with international airports such as Kerala, Delhi, Bengaluru, Chennai and Mumbai were the first hotspots in India, due to imported infection, he explained. Hotspots are determined by the number of people in the community, their social mixing pattern and the introduction of infection, and with each ‘unlock’, as movement of people within and across states increased, the virus spread in more districts.
“Many are worried only about the rise [of COVID-19 cases] in certain cities but are not paying attention to the silent areas that are high in population. These areas are more dangerous and are likely to become future hotspots.” Babu said. “It is only a matter of time.”
Take, for instance, Maharashtra. In April, the MoHFW identified 11 districts as hotspots in the state. As of September 20, 27 municipal corporations--under 20 districts--fell under ‘red’ zones categorised as hotspots, as per an analysis by the Medical Education and Drugs Department of the Maharashtra government. India’s central health ministry says that a hotspot is classified based on total active cases, doubling time of confirmed cases and testing and surveillance feedback.
We analysed data to identify which districts have a high spread of the disease in the population and are at danger of a surge in cases. We used the test positivity ratio (TPR)--the proportion of positive samples in all tests done until that date--and the doubling time of COVID-19 cases in six weeks to September 20 to categorise districts as hotspots. We used data from COVID-19 India, a crowdsourced database of COVID-19 data, and data from MoHFW. Data on doubling time are available for all districts while data on testing were available for 16 districts in Maharashtra, seven in Karnataka and for all 13 in Andhra Pradesh. Even these 36 districts have patchy testing data with data missing for one or several days. Further, we excluded districts with a gap of seven consecutive days or more.
Overall, India had an average TPR of 8.52% and a doubling time of 48 days as of September 22. An area’s COVID-19 TPR should be below 5% in the last two weeks for it to be deemed to be controlling the virus, according to the World Health Organization (WHO).
If a district consistently has a TPR greater than 5% or a TPR that is increasing, it is likely that the virus is spreading and the district is not testing enough people, said Gautam Menon, professor of physics and biology at Ashoka University in Haryana. Because the district is not testing enough, COVID-19 cases are not identified and isolated in time, which will result in more cases in the future.
On March 6, the WHO said that 80% of COVID-19 infections were either mild or asymptomatic, which might make these cases difficult to catch, unless there is extensive testing. Unlike the test positivity rate, doubling time does not have an official definition or a cut-off number. A short doubling time means that cases are increasing exponentially and could burden the healthcare system. The districts most at risk are those that have a high or increasing TPR as well as a short doubling time.
Of the 36 districts analysed, none has a TPR below 5% and three districts have doubling times less than 20 days, our analysis shows. Many other factors help discern a hotspot but these two indicators are a good measure of a district's success in controlling the epidemic. A doubling time under 20 suggests that the district is vulnerable, said Menon.
Only four districts--Wardha (9.4%) in Maharashtra, Kodagu in Karnataka (6.3%), and Krishna (5.7%) and Srikakulam (9.3%) in Andhra Pradesh--have a TPR under 10%, but the rate is rising in all of them.
Gondia (14 days), Yavatmal (15 days) and Wardha (16 days)--all in Maharashtra--have a doubling time of less than 20 days. Of these, Gondia also has a high TPR of 17.5%. “This is a worrying trend. Any district with a TPR close to 20% and a doubling time below 20 days needs immediate attention,” said Menon.
Kodagu in Karnataka has a low TPR of 6.3% and a high doubling time of 41 days. Similarly, Krishna in Andhra Pradesh has a TPR of 5.7% and a doubling time of 36 days.
The third scenario we found was when a district with a long doubling time--such as Pune, Mumbai and Thane--also has a high TPR. One of the reasons for this could be that these districts are testing more, including those who might not have been tested under earlier guidelines, and are likely picking up more asymptomatic cases than before, said Menon. This would, in the long term, reduce the stress on the healthcare system as even asymptomatic cases can be isolated and prevented from spreading the infection further, he explained. But he cautioned that testing in India is yet to reach the level where most cases can be found in time. If the TPR is consistently high, these districts too should be considered as hotspots, said Menon.
Maharashtra
All 19 districts in Maharashtra for which data are available are hotspots, based on TPR and doubling time.
Pune has the most active cases (74,768)--higher than all confirmed cases in Portugal (68,577)--as of September 20. Its TPR has consistently been higher than 20% and has increased from 23% on August 10 to 25% on September 20. Mumbai’s doubling time has decreased from 83 days on August 10 to 64 days on September 19, while its TPR has remained high at 18%. This is a worrying trend, Menon said.
The influx of COVID-19 patients to Mumbai’s hospitals from outside the city and state had strained the availability of hospital beds, Gautam Bhansali, general medicine and infectious diseases specialist at Bombay Hospital, and the chief coordinator between the city’s civic body and its private hospitals, told IndiaSpend.
All of Maharashtra’s districts have a TPR above 10%, except Wardha (9.4%). Raigad has the highest (32.2%). The epidemic is spreading faster in Gondia, Yavatmal, Wardha and Nagpur, where the doubling time is low and the TPR high and increasing.
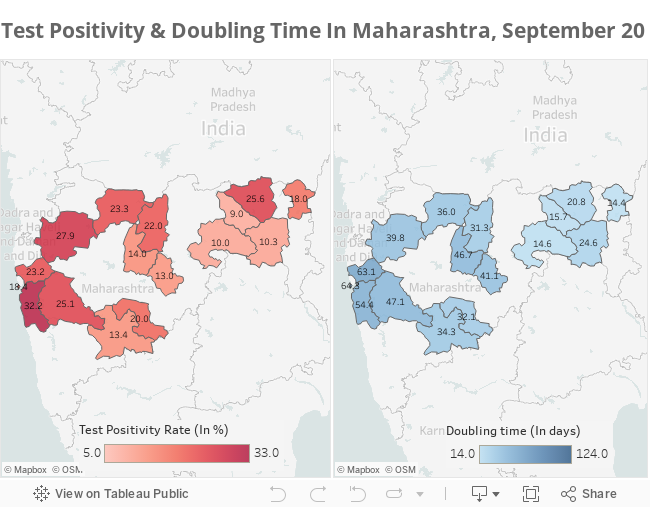
Source: www.covid19india.orgNote: Doubling times are three-day averages centred on September 19
Karnataka
Although Bengaluru Urban is the second-worst affected district in the country, based on the number of active cases (41,754) on September 20, the spread of the virus seems to be slowing in the city--its TPR declined from 18% on August 10 to 14% on September 20 while its doubling time rose from 27 days on August 10 to 38 days on September 19 (three-day average). The city remains a hotspot because the TPR is over 5%.
Six of the seven districts analysed in Karnataka have a TPR above 10%. Kodagu (6.3%) and Kalaburagi (11.7%) have the lowest TPR in the state, but the rate is increasing even as their doubling times have increased over six weeks to September 19 (three-day average).
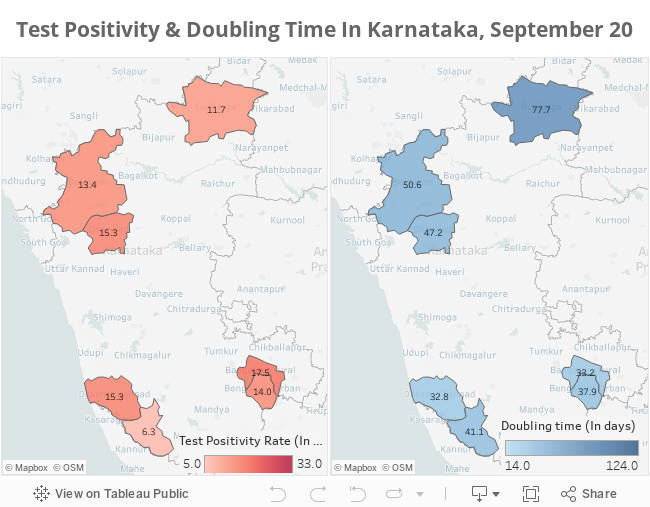
Note: Doubling time is three-day average centred on September 19, except for Belagavi where it is centred on September 13 for lack of later testing dataSource: www.covid19india.org
Andhra Pradesh
Andhra Pradesh is the only state to report more than 20,000 confirmed COVID-19 cases in every district. East Godavari has the highest TPR which increased from 13% to 17% between August 10 and September 20. Over the same period, its doubling time has increased from 18 days to 45 days on August 19.
The district of Krishna has the least TPR (5.7%), rising from 4.3% on August 10. Over the same period, its doubling time increased from 23 to 36 days.
While the doubling time of Kurnool has increased from 23 to 124 days between August 12 and September 19, its TPR has remained constant between 10-12%. This shows that the district is managing to keep the epidemic under control, especially if the TPR drops in the coming month, said Menon.
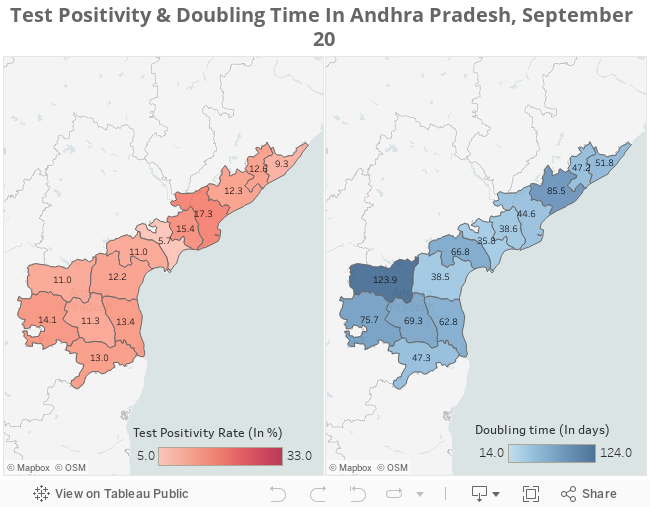
Source: www.covid19india.orgNote: Doubling times are three-day averages centred on September 19
How can districts prepare for a surge?
“Containing spread is ambitious but it can be done if initial infections are detected and contact-tracing and quarantine are aggressive and efficient,” John said.
Chains of asymptomatic transmission--which seems to be the major mode of spreading the infection--can mean that it can be a while before the disease surfaces, especially in the absence of widespread testing, explains Menon. This means that on the individual level, physical distancing has to continue and will likely be the “new normal for a while to come”, he added.
Communities with elderly populations must be protected by ‘reverse quarantine’ at home, John said. This means that those who are vulnerable to serious COVID-19 infections, such as the elderly and those with comorbidities, should stay at home as far as possible and reduce contact with the general population, such as the youth, who are more likely to contract the disease because they are a larger part of the workforce. As many as 57% of 15,962 COVID-19 deaths by July 2 were of those with comorbidities, reported ThePrint based on an analysis by the Integrated Disease Surveillance Programme (IDSP). Of those who died, 52% were above 60 years, the report said.
Each district should have a task force consisting of the district magistrate or collector, the chief medical officer and chief of police as well as representatives of businesses, institutions and non-governmental organisations, said John. The task force would plan for clinical management, screening and treatment of COVID-19 and share lessons from its COVID-19 response across the state, John said.
The state government and district task forces should be prepared to check for symptoms, such as fever, cough and declining oxygen saturation, of those in rural areas, as rural communities near semi-urban areas are vulnerable to COVID-19, said John. Healthcare institutions in urban and semi-urban areas should be ready to take in any symptomatic persons from villages and small towns, he added.
Districts can also prevent a rise in cases by making testing more broadly and easily available, encouraging self-isolation wherever possible and ensuring that treatments for other chronic diseases and immunisation programmes are not neglected, said Menon.
Better medical infrastructure including additional oxygen beds in hospitals and a larger health workforce would help provide the care people need, said Babu of PHFI. “Every district needs a workforce for identification of cases and immediate isolation. This is the only way we can prioritise saving lives.”
(Jacob is an intern with IndiaSpend. Shreya Khaitan edited this story.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
