Why Vulnerable Tribes, Susceptible to Illness, Malnutrition, Have Limited Healthcare

Pallahara, Odisha: In the lush green forest in Pallahara block, Odisha, 16-month-old Babloo Saunto, held in his mother's arms, looked visibly emaciated and frail, unlike most kids his age. The child was recovering from brain malaria, which gave him a month-long fever, violent chills, vomiting and diarrhoea.
With no community health centre in the village, Sukanti Saunto, Babloo’s 28-year-old mother embarked on a 90 km journey to the nearest district hospital in Keonjhar. The Sauntos belong to the Pahadi Bhuyan (literally, hill tribe), one of Odisha’s 13 particularly vulnerable tribes--the most disadvantaged of all of India’s recognised tribes (known as scheduled tribes), living in isolation, deep in the hills of Pallahara.
“In the absence of health care services and lack of transportation, vulnerable tribes are deprived of timely health care facilities,” according to a 2017 report by the Comptroller and Auditor General (CAG) of India. These problems are exacerbated by a lack of a stable income, low nutrition, limited access to child care centres and rising food insecurity, an IndiaSpend investigation found.
Tribal groups--that are more vulnerable to disease and malnutrition than the rest of the population--have to cover a distance of five to 80 km to reach a community or district health centre, the 2017 report CAG report said. Across India, people have to cover an average distance of 13.55 km to reach a community health centre.
Though nutrition and health outcomes of scheduled tribes have improved over the past three decades, they still perform poorly when compared to the rest of the population. Tribals constitute 8% of India’s total population, but, in 2015, they accounted for 30% of all cases of malaria, including brain malaria, and 50% of deaths because of malaria. This has an economic burden of Rs 6,000 crore, according to the 2018 tribal health report by the Ministry of Health and Family Welfare.
Of 75 particularly vulnerable tribal groups across the country, Odisha, with 13 vulnerable tribes, has the most. These groups--with a total population of 89,208--are spread over 12 districts of Odisha, according to the National Centre for Advocacy Studies.
The Pahadi Bhuyans, with a population of 5,578, qualify as a vulnerable tribe because of their stagnant population, low level of literacy and pre-agricultural level of technology, according to a 2013 report by the Ministry of Tribal Affairs.
Lack of data
There are no data on development outcomes of particularly vulnerable tribal groups, such as the Pahadi Bhuyan in Odisha. These groups are worse off than other scheduled tribes and their health remains severely neglected, according a 2014 report by the Xaxa Committee, set up by the tribal ministry on particularly vulnerable tribal groups.
There is a “near complete absence of data on the health situation of tribal different communities”, the 2018 tribal ministry report said.
Even the National Family Health Survey (NFHS) data for scheduled tribes could be underestimations, as they are based on a small sample size, according to the 2018 tribal ministry report.
In 2015-16, the infant mortality rate (IMR)--child deaths, under one year, per 1,000 births--in scheduled tribes was 44.4, 30% higher than that of the rest of the population (32.1), excluding scheduled castes, scheduled tribes and other backward classes, data from the NFHS show.
Based on their estimations, the 2018 ministry report says that India’s IMR could be anywhere between 44.4 and 74 deaths per 1,000 births for scheduled tribes.
Over a decade to 2015-16, the IMR for scheduled tribes decreased more rapidly than that for the rest of the population. In 2005-06, the IMR for scheduled tribes was 62.1, compared to 38.9 for the rest of the population, NFHS data show.
Health centres understaffed, too far
Charad Saunto, 32, Babloo’s father, like others in the Pahadi Bhuyan tribe, practises shifting cultivation, and has no stable income. Eventually, Charad Saunto had to borrow money from a private money lender to pay for his son’s medicines. “The doctor prescribed medicines worth Rs 800. I will have to pay the moneylender Rs 1,500 back,” said Saunto.
The insecure livelihoods, and lack of access to government services, have grave consequences for the health of scheduled tribes. For instance, “parents take their children, as young as one-year-old, to the jungle to collect food, and expose them to diseases that could kill them”, such as malaria, dengue and other mosquito-borne diseases, said Dhanumati Dehuray, 35, sarpanch (village head) of Bauradiya village, inhabited by the Pahadi Bhuyan tribe.
Healthcare is too far from the village, and often of subpar quality. The Sauntos had to travel, as we said, 90 km to the nearest hospital to get Babloo treated.
As many as 82.3% of specialist positions in community health centres, 32.6% of technician positions, and 27.9% of nurse posts in community and primary health centres in tribal areas were vacant in 2017, the 2018 tribal ministry report said.
Tribal populations are more malnourished
In 2009-10, the proportion of the scheduled tribe population living below the poverty line in rural India was 47.4%, compared to 33.8% across India. In urban areas, the proportion was 30.4% for scheduled tribes and 20.9% for the entire population.
The Sauntos travel 12 km, a two-hour journey on foot, to the nearest fair-price shop to access their monthly rations from the public distribution system, as this is the closest centre with fingerprint authentication. On their way back, they lug 35 kg of ration through the rugged hilly terrain.
The daily intake of nutrients by tribal groups is below the recommended daily level and has reduced over the years, indicating rising food insecurity among the tribal populations, according to the ministry of health’s 2018 report. Particularly vulnerable tribal groups are identified as the most susceptible to malnutrition, according to a 2008 government report.
Since 1975, the government has a supplementary nutrition programme, under the Integrated Child Development Services, which provides take-home rations--chhatua, eggs and pulses in the case of Odisha--for pregnant women, lactating mothers and children, along with providing hot cooked meals for children, three to six years, at anganwadi centres, as reported by IndiaSpend in August 2019. This helps support a child’s first 1,000 days--a window of opportunity in early childhood when a child’s growth and cognitive development is maximum.
Babloo Saunto’s mother collects take-home rations of chhatua, eggs and pulses once a month from the village anganwadi centre, but her older son, now 5, does not get hot, cooked meals as the anganwadi is too far away to go to everyday.
The anganwadi centre was shut the day IndiaSpend visited, and it is rarely open, villagers told us.
“I could not open the anganwadi today because I had to go to the Child Development Office in Pallahara block, 50 km away, for the registration for new Mamata beneficiaries”--a direct cash transfer programme for pregnant mothers, said Mundaram Pradhan, 45, the anganwadi worker, who insisted that the centre was shut only that day.
In 16 months, they have gone twice to the village health nutrition day, where children are vaccinated, given regular doses of vitamin A, and dewormed. It is supposed to be organised once every month at the anganwadi (child care) centre in the village. “We are not aware and neither are we informed when village health nutrition days are organised,” said Sukanti Saunto.
The closest anganwadi centre is 3 km from the Sauntos’ village; centres have not been set up in 226 particularly vulnerable tribal group villages in Odisha, data from the 2017 CAG report showed. Sixteen villages are between 3 and 8 km away from the nearest anganwadi centre, according to the report.
In 2013, 19 infants died due to malnutrition, when the Odisha government ran a special project for the development of the vulnerable tribal groups, and set up the Paudi Bhuyan Development. Under the project, 216 children were identified as severely underweight and suffering from severe acute malnourishment, but 60 of these were not referred to any hospital, found the 2017 CAG report, the latest on particularly vulnerable groups. “No remedial measures were taken by micro-projects to eradicate malnutrition,” the report said.
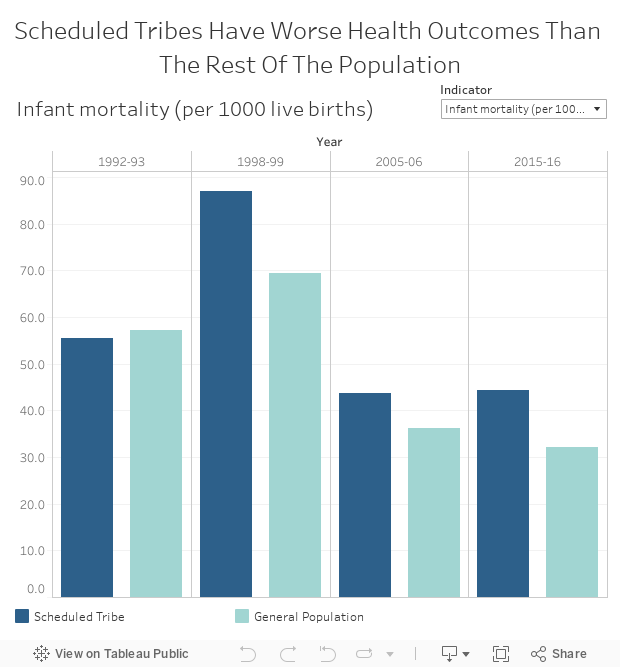
Source: NFHS 1, NFHS 2, NFHS 3, NFHS 4 and 2018 Tribal Health Report by the Ministry of Tribal Affairs
Note: 1. Health indicators for scheduled tribes in 2015-16 are an estimation and have been calculated from districts where more than 50% of the population belongs to Scheduled Tribes.
2. ‘General Population’ excludes scheduled castes, scheduled tribes and other backward castes.
Funds earmarked for non-targeted schemes
There is a dedicated fund for the welfare of tribals linked to their proportion in the population that cannot be allocated elsewhere.
Under the National Democratic Alliance government headed by the Bharatiya Janata Party, tribal sub-plan expenditure dropped from Rs 32,387 crore in 2014-15 to Rs 20,000 crore in 2015-16 and to Rs 24,005 crore in 2016-17, as IndiaSpend reported in April 2019. The allocation increased to Rs 31,920 crore in 2017-18, but the government allocated money to non-targeted (generic/administrative) expenditure (such as grants towards infrastructure maintenance, farm loan waivers, Good Governance Fund, Sports Authority of India allocations, etc.), which do not go towards the scheduled tribe population, a Dalit Adivasi Budget analysis by the National Campaign on Dalit Human Rights-Dalit Arthik Adhikar Andolon showed.
In 2019-20, a total of Rs 52,885 crore was allocated by the central government for the tribal population. But less than half (40.9%) was for schemes targeting the tribal population, the Dalit Adivasi Budget Analysis found.
| Of Total Budget, Rs 31,257 Crore For Schemes Which Don’t Directly Benefit Scheduled Tribes | |
|---|---|
| Central Government Budget for Scheduled Tribes | Allocation in Rs (crore), 2019-2020 |
| Due budget for central schemes and centrally sponsored schemes targeted to STs | 76,592 |
| Allocation to schemes targeted towards STs | 21,628 |
| Allocation to Non Targeted Schemes | 31,257 |
| Gap in allocation between prescribed allocation to targeted schemes and actual allocation | 23,707 |
Source: Dalit Adivasi Budget Analysis, 2019-2020, National Campaign on Dalit Human Rights-Dalit Arthik Adhikar Andolon
“The weakening of the delivery institutions in the tribal areas have created a self-perpetuating cycle of poor performance, low financial allocations, which in turn, result in low expenditure under centrally sponsored schemes and poor delivery of goods and services, leading to lower subsequent allocations,” according to the 2014 Xaxa Committee report.
For instance, in 2014, Rs 56.17 lakh was released by the women and child development department to the scheduled castes and scheduled tribes department of Odisha to address special health and nutritional needs of vulnerable tribes. But the department did not use this money because of a shortage of manpower, and it was refunded to the women and child ministry in April 2015, found a 2017 CAG report.
Of the Rs 4.28 crore budgeted in 2014 for conducting health camps for vulnerable tribal groups, only Rs 6.25 lakh was used, the report found.
This story was first published here on Healthcheck.
(Ali is an IndiaSpend reporting fellow.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
