Why India Must Move Policy Away From Population Control

New Delhi: As India prepares to become the world’s most-populous country by 2024, family planning--the ‘Family Welfare’ in the Ministry of Health and Family Welfare--continues to get a dominant share of funding and policy attention, leaving fewer resources for overall health system development.
In roughly five years, or by 2024, the population of India is expected to surpass that of China, according to this 2017 United Nations (UN) projection. China’s population will peak at 1.44 billion in 2029 and start declining. As per current estimates, due to what is called population momentum--a higher proportion of people in the reproductive age group--as well as higher life expectancy, India’s population will only peak in the 2060s, before it starts to decline.
However, Indian fertility rates are declining quickly, and some of these estimates are being revised constantly. For example, according to earlier UN estimates, India was to overtake China in 2022. Ten years ago, India had a total fertility rate (TFR) of 2.68; today, according to the National Family Health Survey-4 (NFHS 4), out of 36 states and UTs, only four--Uttar Pradesh (UP), Bihar, Meghalaya and Nagaland--have a TFR more than or equal to 2.68.
India was the first country in the world to formulate a National Family Planning Programme in 1952, with the objective of "reducing birth rate to the extent necessary to stabilise the population at a level consistent with requirement of national economy". The current TFR, at 2.2, is close to the replacement-level fertility rate of 2.1. According to NFHS-4, TFR has declined considerably and between 1992-93 and 2015-16, it declined by 1.2 children (from 3.4 children in 1992-93 to 2.2 in 2015-16).
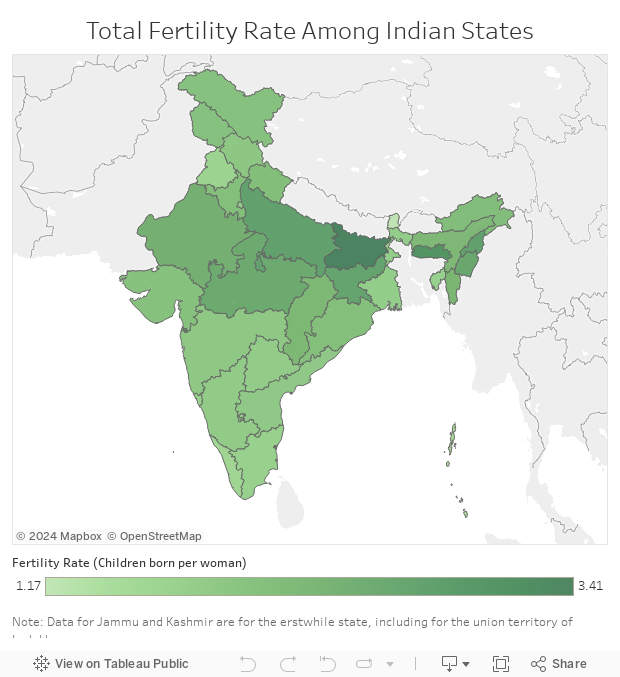
Source: National Family Health Survey, 2015-16
It is often said that “development is the best contraceptive”. The two-pronged approach of health system strengthening and population control may still work in states such as Bihar and UP, but for other states that are near or under replacement fertility, more resources should move into health system strengthening and core health priorities--communicable diseases, drug availability, and human resource deployment, to name just a few. A low child mortality rate and accessible health services would be good incentives for family planning.
This is one of many decisions facing India’s public healthcare sector that this second story under an IndiaSpend-Observer Research Foundation (ORF) series highlights, which the new government must address. Healthcare has received unprecedented attention from political parties during the ongoing elections for the 17th Lok Sabha, even as better measurement, greater evidence and more informed reporting begin to expand voter awareness and deepen policy debates, as we argued in our previous story.
Here are some of the crucial areas on which India must focus more attention, efforts and funds.
Child and maternal mortality rates
However, India’s achievements in preventing child deaths have not been as spectacular, mostly because of meagre fund allocation, over the decades.
When it comes to child mortality, Kerala (ruled by a coalition let by the Communist Party of India-Marxist, CPIM+), Punjab (Congress+), Tamil Nadu (All India Anna Dravida Munnetra Kazhagam, or AIADMK) and Maharashtra (Bharatiya Janata Party and allies, or BJP+) have already attained the National Health Policy (NHP) 2017 neonatal mortality rate target of 16 deaths per 1,000 live births, ahead of the 2025 deadline.
Kerala (CPIM+) has achieved the Sustainable Development Goals 2030 target of 12 deaths per 1,000 live births.
On the other hand, Odisha (Biju Janata Dal, or BJD), Madhya Pradesh (Congress+), Uttar Pradesh (BJP+), Rajasthan (Congress+) and Bihar (BJP+) still have very high neonatal mortality rates.
The Niti Health Index provides state-level scores and ranks for health indicators, and uses the Sample Registration System (SRS), which tracks deaths and births in a sample of villages and urban blocks but does not provide data on infant, child or maternal mortality (NMR, U5MR, MMR and IMR) for eight smaller states and seven UTs.
The National Family Health Survey 2015-16 (NFHS-4) offers data for almost all states and UTs, and shows that over the last decade, under-five mortality rate (U5MR) came down from 74.3 to 50 and infant mortality rate (IMR) came down from 57 to 41, both per 1,000 live births.
The rate of decline, however, was much slower than that of maternal mortality ratio (MMR).
The global U5MR target--collectively set by the UN--is 25 per 1,000 live births by 2030, and according to NFHS-4 (2015-16), only Kerala (CPIM+), Goa (BJP+), Andaman & Nicobar Islands (UT), Puducherry (Congress+) and Lakshadweep (UT) have an U5MR lesser than 25. (Union Territories are normally governed directly by the President through an administrator. However, the National Capital Territory of Delhi and Union Territory of Puducherry each has a legislative assembly and a council of ministers.)
Manipur (BJP+), Tamil Nadu (AIADMK) and Maharashtra (BJP+) are close to achieving the target with an existing U5MR of under 30. Despite being better performers in health indicators on an average, Delhi (AAP) and Himachal Pradesh (BJP+) are the only states (for which data are available) whose progress over the last decade has been insignificant or negative.
Himachal Pradesh, which was ranked five from the top among 29 states and UTs a decade ago (with a U5MR of 41.5), is now at rank 18 from the top, among 35 states and UTs. Worst has been Delhi’s case where U5MR seems to have worsened over the last decade, and from being in the top 10 performers just a decade ago, Delhi is one of the bottom 10 now, in the company of Uttarakhand, Odisha, Rajasthan, Jharkhand, Assam, Bihar, Chhattisgarh, Madhya Pradesh and Uttar Pradesh.
In terms of percentage reduction in the last decade, the top five performers have been Arunachal Pradesh, Kerala, West Bengal, Odisha and Tripura.
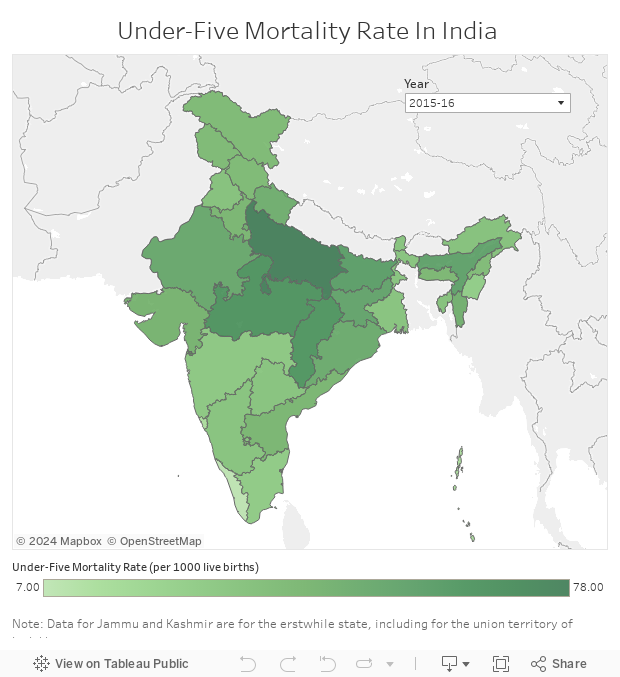
Source: National Family Health Survey, 2015-16
India has less than 15 years to halve its MMR from 130 per 100,000 live births to under 70, in order to meet a global Sustainable Development Goal (SDG) target--MMR lower than 70 by 2030.
Currently, India’s Sample Registration System, which tracks deaths and births in a sample of villages and urban blocks, does not generate data on MMR for smaller states or union territories (UTs). However, historical data on the larger states show most states are doing well. Almost all large states have nearly halved their MMR in the last decade, reducing India’s MMR from 254 to 130.
However, in states such as Punjab and West Bengal, which were among the better performers a decade back, the rates of improvement in MMR have slowed down. Currently, only Kerala (CPIM+), Maharashtra (BJP+) and Tamil Nadu (AIADMK), have achieved an MMR of less than 70 in India.
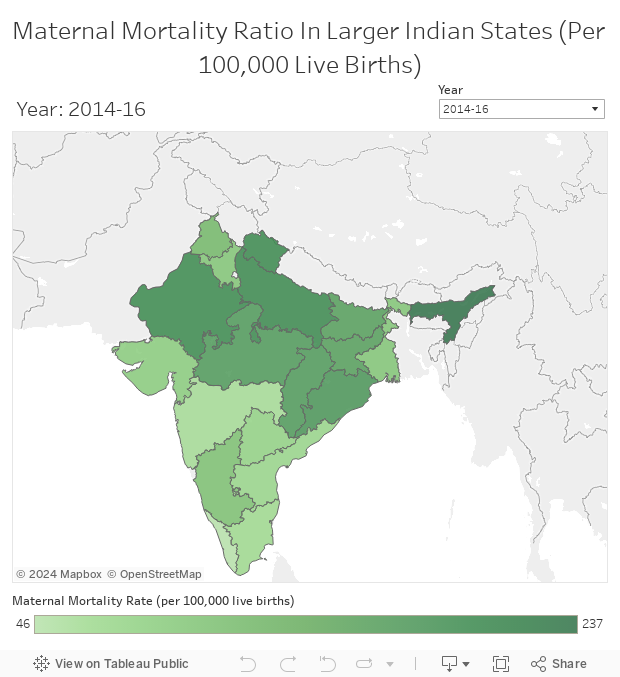
Source: Sample Registration System
Tuberculosis
The Niti Health Index also looks at indicators such as tuberculosis treatment success rate. All the top five states have a success rate of more than 90%: Bihar (BJP+), Rajasthan (Congress+), Madhya Pradesh (Congress+), Mizoram (MNF+) and Jharkhand (BJP+).
Most of the better performing states are also high burden states, and will contribute to India achieving the ambitious ‘TB elimination’ status in the future. According to the Niti data, only three states, Nagaland (BJP+), Sikkim (BJP+) and Daman and Diu (UT), have a treatment success rate of less than 80%.
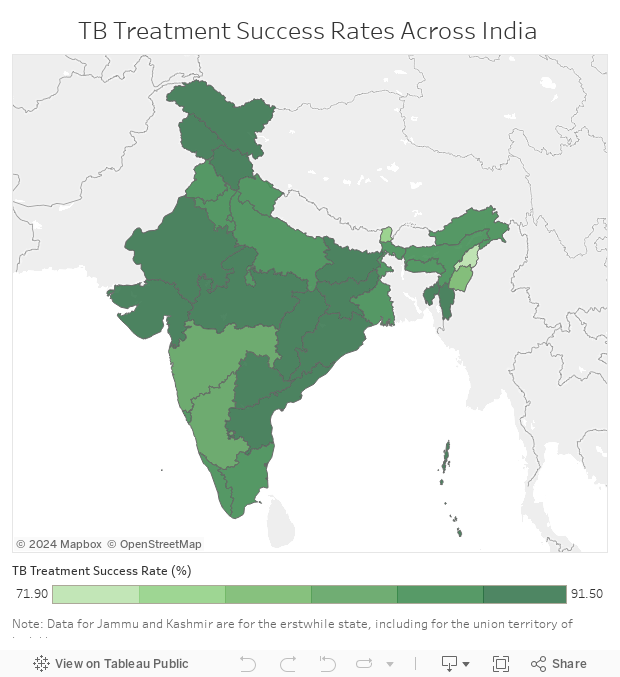
Source: Niti Health Index
Institutional delivery, immunisation
The states which have achieved more than 90% ‘institutional delivery’ (births at a health facility as opposed to at home), according to the Niti Health Index, which depends on the government’s Health Management Information System data, are: Chandigarh (UT), Puducherry (Congress+), Gujarat (BJP+), Mizoram (MNF+), Kerala (CPI-M+) and Goa (BJP+).
Looking at NFHS-4 data, 14 states and UTs, a considerably larger number, are listed as having achieved more than 90% of institutional delivery. The map below uses Niti Health Index data. Only 19 states and UTs have more than 90% of their children fully immunised, according to the Niti Health Index. However, NFHS-4 paints a more sobering picture with only one UT, Puducherry (Congress+), achieving more than 90% coverage in immunisation.
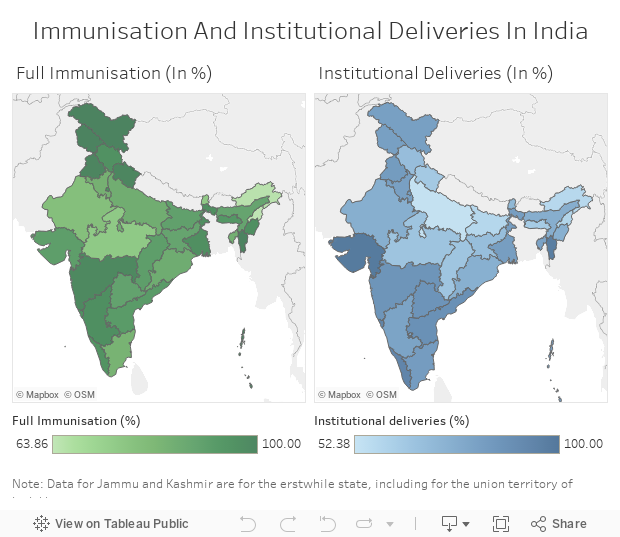
Source: Niti Health Index
One of the biggest drawbacks of the Niti Health Index is that it does not allow for disaggregating health indicators across socio-economic categories. However, using NFHS-4, data can be disaggregated for a select set of indicators. Arguably, the most far-reaching progress over the last decade has been that while wealth-based inequities remain, caste-based inequities in access to institutional delivery and immunisation are fast disappearing due to focused attention by the central as well as state governments.
Perhaps a first in India’s history, Dalits (Scheduled Castes) have a higher proportion of children fully immunised (63.2%) than the national average (62%). However, Adivasis (Scheduled Tribes), Muslims as well as those from the lowest income quintile (the 20% lowest earners) have significantly lower coverage of immunisation, and need focused attention. A similar trend is visible for institutional delivery as well.
In the Niti sub-domain index focused on outcomes and access indicators, Mizoram (MNF+), Kerala (CPIM+), Lakshadweep (NA), Punjab (Congress+) and Jammu & Kashmir (NA, because currently under President’s rule) were the top performers. Among states, Bihar (BJP+), Madhya Pradesh (Congress+), Odisha (BJD), Uttar Pradesh (BJP+) and Rajasthan (Congress+) were the lowest performers.
Shifting focus
Given the remarkable improvement in child mortality rates, and healthcare service access in a context of very little investment in healthcare services, it is an ethical imperative to shift expenditure and efforts away from a narrow focus on family planning--a euphemism for population control--to core health priorities such as communicable diseases, drug availability, and human resource deployment
Currently, only 12 states and UTs, starting with Bihar (BJP+), Uttar Pradesh (BJP+), Madhya Pradesh (Congress+), Jharkhand (BJP+) and Rajasthan (Congress+) have a fertility rate higher than replacement level.
The data show that many of the better performing states such as Mizoram, Kerala and Telangana have been ruled by non-mainstream, regional parties like the MNF, CPI-M or the Telangana Rashtra Samithi. However, barring Odisha (BJD), all the low performing states are under either BJP or INC coalitions. The large parties, as well as the laggard states they have ruled such as Rajasthan, Uttar Pradesh, Madhya Pradesh and Bihar, must step up.
A common minimum programme agreed upon by a multi-stakeholder consensus involving all political parties could be a way forward. It could effectively address misalignment between central and state efforts, as well as delays and derailments due to regime changes.
The next piece will focus on governance issues in the provision of public healthcare, as well as on how synergies must be harnessed in a context of policy fragmentation for the larger public good.
This story was first published here on HealthCheck.
(Kurian is Fellow at Observer Research Foundation’s Health Initiative.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
