Why India Cannot Follow A New WHO Guideline To Protect Its Mothers

India must double antenatal visits by health workers--according to a new World Health Organization (WHO) guideline--to pregnant women to reduce the risk of stillbirths and pregnancy complications.
Is India ready to implement this and other new WHO guidelines to protect its mothers? It is not, according to an IndiaSpend analysis of government data and research studies.
In November 2016, the WHO released this antenatal care model for pregnant women to reduce the risk of stillbirths and pregnancy complications. In 2015, an estimated 0.3 million women died from pregnancy-related causes, 2.7 million babies died during the first 28 days of life and 2.6 million babies were stillborn globally, according to WHO data.
The Indian government, on February 15, 2017, committed to halving preventable deaths of pregnant women and newborns in health facilities over the next five years. It is part of a new network to improve the quality of care for maternal, newborn and child health, announced by the WHO in February 2017. Other than India, the network comprises of Bangladesh, A Cote d’Ivoire, Ethiopia, Ghana, Malawi, Nigeria, Tanzania and Uganda.
These countries will strengthen capacity and motivation of health professionals to plan and manage quality improvement, improving data collection and increasing access to medicines, supplies, equipment and clean water. Through a global learning platform, the network will build a community of health practitioners from the facility level and develop evidence-based strategies to improve quality of care, harvest implementation ideas, and collect information and experiences about what is working.
The quality of antenatal care is vital to reduce the risk of stillbirths and pregnancy complications, and the absence of it explains why more women enrolling for hospital deliveries in India isn’t translating into fewer maternal deaths, IndiaSpend reported in February 2017.
India’s maternal mortality rate (MMR) was 178 deaths per 100,000 live births in 2011-12, worse than Sri Lanka (30), Bhutan (148) and Cambodia (161), and worst among the BRICS countries: Russia (25), China (27), Brazil (44), and South Africa (138), IndiaSpend reported in September 2016.
Government plans for the future, struggles with present
In November 2016, the government launched the Pradhan Mantri Surakshit Matritva Abhiyan, or the Prime Minister Safe Pregnancy Scheme, which aims to provide free and comprehensive care on the ninth day of every month during pregnancy. Pregnant women are provided special, free ante-natal checks in their second or third trimester at government health care facilities, including ultrasounds, blood and urine tests.
Yet, getting these facilities to women is a challenge, especially in poorer states. No more than 3.3% of pregnant women in Bihar reported receiving full antenatal care, lowest among states, followed by Tripura (7.6%) and Rajasthan (9.6%), according to data from the National Family Health Survey (NFHS) 2015-16. Full ANC refers to at least four antenatal visits, at least one tetanus toxoid (TT) injection and iron folic acid tablets or syrup taken for 100 or more days.
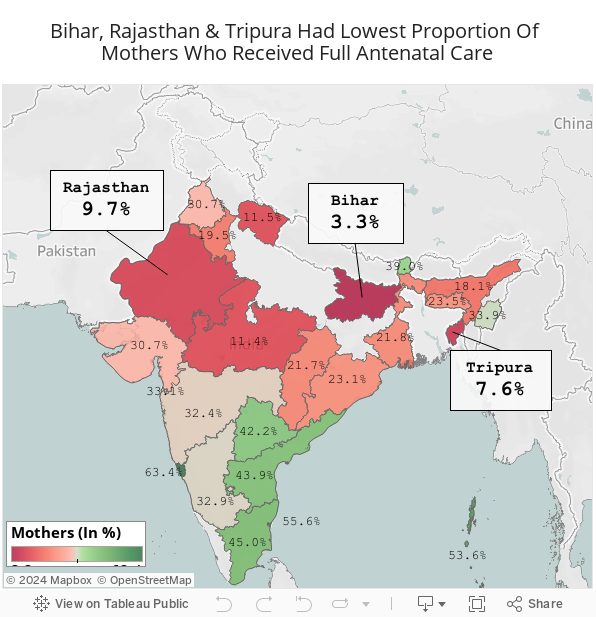
Source: National Family Health Survey, 2015-16
Despite a 62% reduction in child mortality in India between 1990 and 2015, more children (1.3 million) below five died in India in 2015 than anywhere in the world, and India had more stillborn babies than any other country, 26% of neonatal deaths and close to a fifth of 303,000 maternal deaths in 2015, IndiaSpend reported here and here.
IndiaSpend looked at some of the WHO recommendations and evaluated India’s ability to implement them:
1. Minimum of eight antenatal contacts with pregnant women
A minimum of eight contacts for antenatal care can reduce perinatal deaths by up to eight per 1,000 births, compared to a minimum of four visits, said the WHO.
"More and better quality contacts between all women and their health providers throughout pregnancy will facilitate the uptake of preventive measures, timely detection of risks, reduces complications and addresses health inequalities," said Anthony Costello, Director of Maternal, Newborn, Child and Adolescent Health, WHO. "Ante-natal care for first time mothers is key. This will determine how they use antenatal care in future pregnancies."
Despite the emphasis to antenatal care under government health programmes, India is not close to universal antenatal care, according to this 2016 study, which analysed data from the National Sample Survey Office (NSSO).
The study found that women belonging to disadvantaged communities, particularly scheduled-caste (SC), scheduled-tribe (ST) and rural areas, received sparser ante-natal care. SC/ST women contribute to the highest proportion of pregnant women without antenatal care.
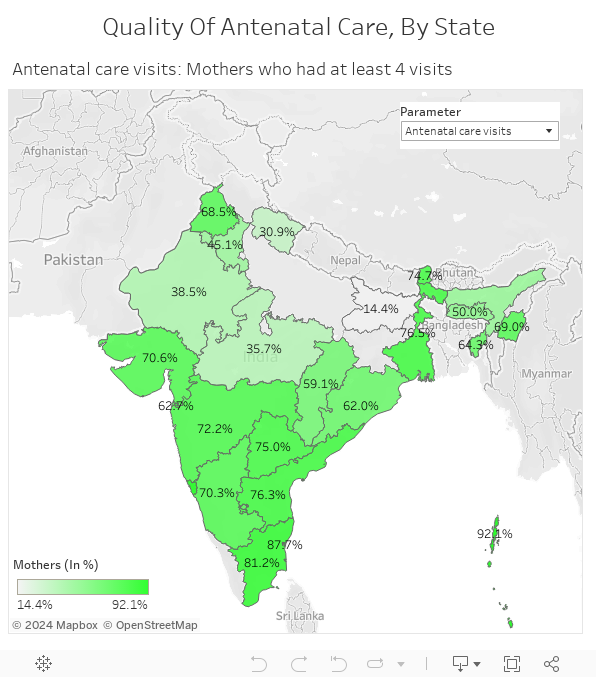
The proportion of mothers who had at least four antenatal visits varied considerably: While states such as Bihar, Madhya Pradesh and Uttarakhand reported four visits to 14.4%, 35.7% and 30.9%, respectively, of mothers, richer states, such as Tamil Nadu (81.2%), Maharashtra (72.2%) and Andhra Pradesh (76%), did better.
Women who received four or more antenatal-care visits were more likely to deliver babies in a health facility, according to this 2016 study, which analysed data from 10 South-Asian countries, including India.
2. Daily oral iron, folic acid supplements
The WHO guidelines recommend daily oral iron and folic acid supplements with 30 mg to 60 mg of elemental iron and 400 µg (0.4 mg) of folic acid for pregnant women to prevent maternal anaemia, puerperal sepsis, low birth weight, and preterm birth.
Anaemia was the top cause of maternal deaths in India (50%) and the associated cause in 20% of maternal deaths, according to this 2014 study in Nutrition, a journal, and India reported that 45% of pregnant women were anaemic--the highest proportion in the world--even though there has been a fall of 12% in the last ten years, IndiaSpend reported in September 2016.
Of all Indian infants who died within 29 days post-birth between 2010 and 2013, 48% were underweight or were prematurely born. At 3.5 million, India accounted for the most preterm births in the world, IndiaSpend reported in November 2016.
Only 9.7% of mothers in Bihar consumed iron and folic acid for 100 or more days when they were pregnant, followed by Tripura (13.4%) and Rajasthan (17.3%), according to NFHS-4 data.
Source: National Family Health Survey, 2015-16
In the 2017-18 budget, the Indira Gandhi Matritva Sahyog Yojna (Maternal Benefit Scheme) saw an increase of 226% in allocation, from Rs 634 crore ($94.6 million) in 2016-17 to Rs 2,700 crore ($298 million) in 2017-18.
This allocation, however, isn’t enough to cover all expectant mothers.
The government had estimated that the the annual requirement for this maternity benefit scheme would be Rs 14,512 crore ($2.1 billion), according to the report of the Standing Committee on Food, Consumer Affairs and Public Distribution (2012-13). “At the rate of Rs 1,000 per month for six months, the scheme expenditure towards maternity benefits to 2.25 crore pregnant and lactating women works out to Rs 14,512 crore per annum,” the report mentioned, the Indian Express reported on 18 February 2017.
Since there isn’t enough funding, the ministry plans to provide maternity benefit only to first-borns.
3. Tetanus toxoid vaccination
The WHO guidelines recommend a tetanus toxoid vaccination for pregnant women to prevent neonatal mortality from tetanus.
India reduced neonatal tetanus mortality by 99.76% over three decades in 2015, which was described as a “significant public health milestone” by the WHO, IndiaSpend reported in October 2015.
In 2013, neonatal tetanus deaths across India fell to 415, from 588 in 2012, but rose to 492 in 2014. Three successive years of meeting the neonatal tetanus elimination threshold of less than one case in 1,000 live births in every district led the WHO to declare India free of neonatal tetanus in May 2015.
However, to mitigate the threat of a resurgence of neonatal tetanus, experts recommend that at least 80% of expectant mothers must be immunised and at least 70% of births must take place in hygienic conditions. Institutional deliveries rose by 15% over a decade from 2004 to 2014, but the rise isn’t translating into fewer maternal deaths, IndiaSpend reported in February 2017.
4. One ultrasound scan before 24 weeks’ gestation
An early ultrasound is recommended for pregnant women to estimate gestational age, improve detection of foetal anomalies and multiple pregnancies, reduce induction of labour for post-term pregnancy, and improve a woman’s pregnancy experience.
Ultrasounds should be done by radiographers at community health centres (CHCs) in rural areas.
CHCs nationwide are 66% short of radiographers, and as many as 13 states and union territories (UTs) are 75% short, according to the Rural Health Statistics (RHS) 2016.
The CHCs constitute the secondary level of health care, providing specialist care to patients referred from primary health centres (PHCs); four PHCs feed into each CHC, serving roughly 80,000 people in tribal, hill or desert areas and 120,000 on the plains.
5. Counselling about healthy eating and keeping physically active during pregnancy
The role of gynaecologists and paediatricians is critical in counselling pregnant women about healthy eating and staying active. However, there is a 77% shortage of obstetricians and gynaecologists and 80% shortage of paediatricians in CHCs nationwide. While 15 states, UTs are more than 90% short of obstetricians and gynaecologists, eight states and UTs said they had no paediatricians.
Nearly 62% of government hospitals--which include CHCs, district hospitals and sub-district hospitals--don’t have a gynaecologist on staff, IndiaSpend reported in September 2016.
There is a link between improved health of the mother and lower stunting among children under five, IndiaSpend reported in January 2016.
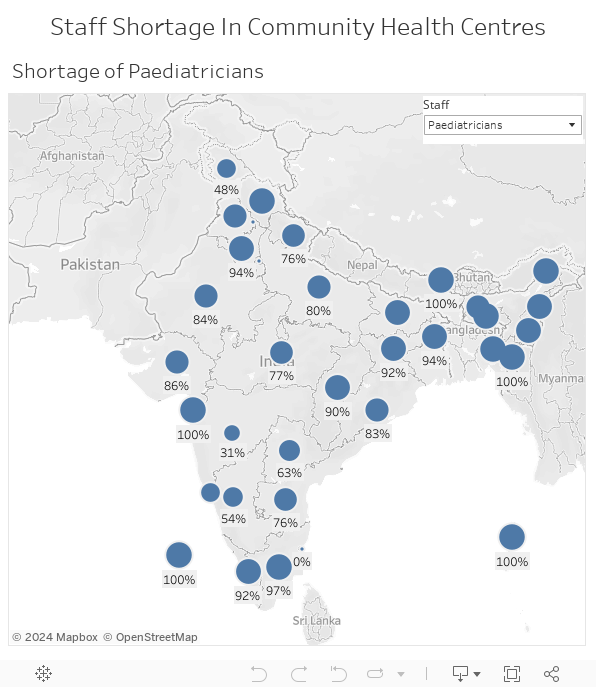
Source: Rural Health Statistics, 2016
6. Health-care providers should ask all pregnant women about their use of alcohol and other substances (past and present) as early as possible during pregnancy and at every antenatal visit
Gynaecologists and auxiliary nurse midwives (ANMs) are the frontline of the battle against infant and maternal mortality and, therefore, their role in ensuring care of pregnant women is critical.
In 30% of India’s districts, sub-centres with ANMs serve double the patients they are meant to and an estimated 22% of sub-centres are short of ANMs, IndiaSpend reported in September 2016.
Maternal cigarette smoking is associated with increased risks for ectopic pregnancy, premature rupture of membranes, abruptio placentae, placenta previa, miscarriage, stillbirth, preterm birth, low birth weight, small for gestational age, and congenital anomalies such as cleft lip.
(Saha is an MA Gender and Development student at Institute of Development Studies, University of Sussex.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
__________________________________________________________________
“Liked this story? Indiaspend.org is a non-profit, and we depend on readers like you to drive our public-interest journalism efforts. Donate Rs 500; Rs 1,000, Rs 2,000.”
