To Work Or Breastfeed: Tough Choice Sets Back Women In India’s Informal Economy

New Delhi: Kavita, a 24-year-old home-based worker, makes toran (decorative wall hangings) for a living. She lives in a north Delhi settlement, working eight hours a day for a daily profit of Rs 30-50.
A tall, streetwise, and seemingly nervous woman, Kavita had to give up a housekeeping job that paid her more than twice her current income because of her childcare responsibilities. She is the primary caregiver for her four-year-old child and a three-month-old infant and also the primary earner in her household. Her husband, a rickshaw driver, hasn’t held a steady job in months, forcing Kavita to juggle responsibilities.
Kavita’s precarious working conditions limit her ability to exclusively breastfeed her infant for six months. Mother’s milk is an important factor in ensuring good health and nutrition among the poorest in a country with a third of the world’s undernourished children under the age of five, according to the Global Nutrition Report 2017.
We asked Kavita if she believed three months of exclusive breastfeeding was enough for her infant. “I managed to do it for three months but I will not be able to do it for six months as one must,” she said. “I have to step out to get a job that pays well and it is unthinkable for me to take my three-month-old child to work with me.”
Kavita’s dilemma is shared by a majority of working mothers in India--they are unable to exclusively breastfeed their infants though they understand its importance, concluded an exploratory research study conducted by the Indian Institute for Human Settlements (IIHS), Bengaluru.
The study surveyed 120 working mothers across three informal professions--domestic workers, street vendors, and home-based workers--through in-depth interviews and group discussions. In India, 81% to 86% of working women are engaged in non-agricultural informal jobs, much like the mothers in this study. They lack maternity protection schemes and paid breaks during work to express and store milk, which can safeguard mothers’ and babies’ interests and health.
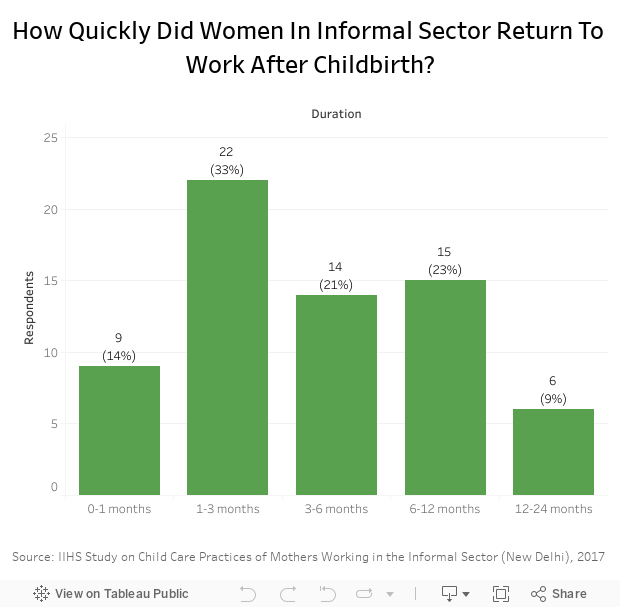
Almost half of the working mothers who participated in our study (47%) returned to work within three months of giving birth, and another 21% would return over the following three months. Of the respondents, 27% could continue to breastfeed exclusively during working hours, while 35% resorted to packaged/powder milk, and 44% fed their infants other fluids as well.
Exclusive breastfeeding is the most effective way to ensure nutrition for the crucial first six months of a child’s life, studies have shown. Without this, children are likely to be stunted--an irreversible condition, which makes prevention key. As many as 48.2 million children in India grow up stunted because of chronic undernutrition during the most critical periods of growth and development in early life, according to the last National Family Health Survey in 2015-16.
Stunting is declining in India with national statistics indicating a decrease of 10 percentage points over the decade to 2016. This is in step with a rise of 8.5 percentage points in exclusive breastfeeding, indicating that still only 55% children are exclusively breastfed for six months.
No maternity protection for mothers in informal sector
Women in formal employment in India are making significant headway in maternity welfare legislation. They are entitled to six-months’ maternity leave for the first two children and the option to work from home when the nature of work allows such an arrangement. This allows them the time to exclusively breastfeed for the required six months.
But informal sector workers have to fend for themselves. For example, they save money to take longer breaks from work after pregnancy, or create care networks using neighbours when there aren’t any creches. But informal sector workers can have their work or earning opportunities taken away from them at short notice, making their work unstable and insecure.
It is unlikely that national breastfeeding and child nutrition targets of increasing exclusive breastfeeding rates to 69% by 2025 can be met equitably given the demographic weight of this population of working mothers.
Kavita is in a doubly precarious situation because her husband is not a dependable earner. In the third month of her newborn’s life, she was forced to look for a second job because her home-based work earned her less than Rs 50 a day which was not enough to cover domestic expenses. While there are public maternity benefit programmes such as Pradhan Mantri Matru Vandana Yojana (prime minister’s programme for mothers, PMMVY) for pregnant women--previously Indira Gandhi Matritva Sahyog Yojana (IGMSY)--there are few schemes to help women who have to work immediately after childbirth.
Thus far, there have been no significant welfare innovations to help mothers working in the informal employment step away from the workforce to adequately breastfeed their children.
With men in unstable small jobs, women become primary earners
The understanding that women’s incomes are supplemental to their husbands’--or are used for non-fixed expenses--is not true for the sampled women. Like Kavita, most women in the study sample are de facto breadwinners or primary earners in dual-earning households. Their income supports household rent, electricity and food costs as well as the costs of education and healthcare. Some women participants reported that they started working to meet the additional costs of having an infant. These women had to go back to work as soon as possible after the delivery because they could not forego the income that supports household subsistence.
“The children come to us when they need books for school, new clothes, some biscuits,” said Janvi, a 23-year-old domestic worker. “They know where the money is--with their mother. Even my little baby, not even two, knows that the money is in my shirt and when she wants Frooti [mango drink], she puts her hand there and asks.”
Three in every five women in the survey reported that their husband displayed irregularity in finding work. Across the three sampled settlements, women’s husbands were out of work, in search of work or underemployed, often making women the sole stable earners of the household. This irregularity in work and income was due to the lack of daily-wage jobs in construction, the seasonal nature of self-employed work such as catering or electricals management for weddings or disruptions in small vending businesses caused by licensing issues.
Despite these disruptions, in our interviews with the women, we found that their husbands were not inclined to acquire new skills that could get them regular or more stable jobs. This meant that women were often the sole stable earners in their households who could not afford to take time off after childbirth.
“It’s like they [the husbands] don’t care if they don’t have work for 5-10 days or even two months,” said Renu, a 26-year-old vendor. “I know if I don’t work for five days there will be no milk for tea the next morning, and no roti to eat at night. Even if your body hurts, you have to get up and go to work.”
For men, the monetary cost of acquiring new skills or aspiring to better work in a mega city labour market was too high to make it a viable choice, we found.
These factors are specific to megacities such as New Delhi which have become uninhabitable for semi-skilled residents forcing them out of any kind of regular work even in the informal sector. This exclusionary urbanisation forces women into gender-segregated work sectors such as domestic work and home-based work to become de facto head earners for their households.
Early weaning often led to digestive problems and undernourishment
Women in the study did not know how to construct the best nutrition for their infants or find other ways to cope with the challenges of poor working mothers even though they had good access to public and private healthcare options during and after pregnancy. They missed the opportunity to ask healthcare workers, families or community members how to manage breastfeeding, food, and work because they were unable to acknowledge just how much they worked, and how little time they could devote to their infants. Working mothers fashioned feeding patterns with insufficient information, leading to lower nutritional outcomes for their infants.
Mothers weaned their infants off breastmilk so that they could get back to work. In most cases, this led to children receiving inadequate feeds as mothers reported that they were unable to afford infant formula as a regular supplement.
“Ek baar bachche ko maa ke doodh ki aadat ho jaaye toh bahar ka doodh shuru karna mushkil ho jata hain. Isliye 12-14 din mein hi bahar ka doodh shuru kar deti hu (If a child gets used to only breastmilk it is difficult to get them habituated to other milk, so I start feeding other milk within 12-14 days of birth),” said Devi, a 22-year-old street vendor.
Infants were fed buffalo and cow’s milk, along with porridge and pulses, at a time when their digestive systems had not yet fully developed. This caused persistent diarrhoea--another common trend amongst children who were undernourished and at risk of stunting and wasting.
Infants being given water, critical source of many infections
To counter diarrhoea, mothers often thinned buffalo or cow’s milk, or fed the infants tea or juice using unfiltered and untreated water much against global nutritional guidelines for babies under six months of age. In all these alternate feeding options, water introduced a critical source of infection in infants at an age where the baby’s gut was still forming. With sub-optimal environmental sanitation and lack of clean drinking water in many of the settlements where such informal workers live, the chances of water-induced diarrhoea--the third leading cause of mortality among children under the age of five--are very high as reported in the National Family Health Surveys.
“Paani ubaal ke nahi dete, itna dhyaan nahi de paate bachche ko. Jab bohot ganda ho toh ubaalte hain. Kuch alag se banaye bachche ke liye, itna time hi nahi ho pata. (I don’t boil the water I feed my child because I do not have the time to be so careful. If it’s visibly unclean, I do. I don’t have the time to make specific food preparations for my child),” said Lakshmee, a 22-year-old domestic worker.

The open drainage and taps supplying drinking water that line the alleys in one of the informal settlements in north Delhi sampled in the study. Poor hygiene and lack of clean drinking water increase the chances of water-induced diarrhoea--the third leading cause of mortality among children under the age of five.
Workplace offers little or no support for breastfeeding
Home-based workers like Kavita came the closest to being able to exclusively breastfeed their infants because they did not face the issue of transporting their children to worksites. Street vendors and domestic workers found this extremely challenging for reasons that are specific to their sectors of work.
Vending in the open is a physically demanding job requiring vendors be alert and engage the customers for every sale. Working mothers in this sector cannot attend to their infants during peak market hours, and do not easily find safe spaces to keep their infants.

Vending in the open is a physically demanding job that needs constant attention and presence, allowing new mothers little time to care for their infants. The women in the photograph was vending within 100 m of her house, allowing her to visit her child frequently. A young girl from the family network takes over when the former takes a break.
Domestic workers must seek permission to bring their infants to the houses of employers. Employers often do not give permission because they fear that children will dirty their house, break fragile objects and distract their mothers.
When bringing a child to work is not an option, mothers have to make alternative arrangements to balance work and care. Kavita could not retain her job as housekeeping staff because she could neither find a safe place for her infant at work nor a caregiver at home. She could only find an eight-year-old girl in her neigbourhood to babysit her child. Though Kavita lived in a large joint family, all the women in her family worked. Her neighbourhood creche did not accept children younger than 10-12 months of age.
The oft-cited solution to breastfeeding while working--expressed breastmilk--wasn’t an option for working mothers in Delhi. There were significant cultural barriers against pumping and expressing milk. Mothers thought breast milk would spoil as soon as it left their breast. They also mentioned having to seek permission from their in-laws or husbands to express milk. The absence of access to a fridge or any cold storage at their home or workplace for storing expressed breastmilk was also a deterrent.
Women left to juggle multiple roles with no support systems
There is evidence to suggest that women use the flexibility of informal work to manage the triple burden of work, household chores, and caregiving. These conditions still make them vulnerable to exogenous shocks. There is a tension between their need and desire to improve their household’s economic standing and their ability to breastfeed in inadequate workplace and employment conditions.
In the face of urgent economic and livelihood responsibilities women such as Kavita face, exclusive breastfeeding isn’t a priority. To expect one to pursue optimal breastfeeding patterns in such circumstances is to forget that the mother is also a worker. It is also asking an individual to fill the gaps for structural issues of lack of social protection, lack of decent work and employment, and inadequate environmental sanitation.
As taking off from work seems impossible to the women in the study, they were interested in an improved communication programme around breastfeeding, one that goes beyond the advisory and operational details, and shares more information on the scientific aspects of it. This, they say, may allow them to fashion more informed feeding patterns.
(Chowdhury and Surie are part of the academics and research team at the Indian Institute for Human Settlements. They work on social protection, the informal economy and urban health.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
