National Teen Health Programme Could Help Millions--If They Knew About It

Sitapur, Uttar Pradesh: “Girls in the village are very hesitant to talk about personal hygiene and sexual health,” said Sheetal Raj, a second year Bachelor of Arts student, and a resident of Sameesa, a village in Sitapur district in Uttar Pradesh (UP), 90 km north of Lucknow, the state capital. “I find it hard to get them to attend community meetings on menstrual health."
Sheetal Raj is a peer educator in the government’s Rashtriya Kishor Swasthya Karyakram, the national adolescent health programme, launched in 2014. In a country where it is often a taboo to even talk about menstruation, Sheetal Raj is one of UP’s 33,989 sathiyas or peer educators--both boys and girls--who educate 10-19 years about pubertal changes, personal hygiene, sanitation and menstrual health.
In India, where 58% women used a hygienic method of menstrual protection such as sanitary napkins and 27% were married before the age of 18 years in 2015-16, such peer educators have emerged as local leaders, and are confidants that young girls can speak to about problems they would have otherwise not discussed with anyone.
Though the programme is a first step in creating more awareness about menstrual and adolescent health in general, it still has several problems: many adolescents are unaware of such a programme, peer educators receive little training and support, the quality of counsellors is poor, adolescent health clinics, and subsidised sanitary napkins, are still inaccessible for many children, an IndiaSpend investigation in UP’s Sitapur district found.
More than 33% of the disease burden and almost 60% of premature deaths among adults can be associated with behaviours or conditions that begin or occur during adolescence, according to a 2014 report by the World Health Organization. If India is able to improve adolescent health for the country’s 236.5 million children between the ages of 10 and 19 years, it will create a healthier and more productive working population that can benefit the country’s growth and development.
Further, with spending on adolescent health, India can avert 35,000 maternal deaths and 1.2 million infant deaths while saving more than Rs 4,450 crore, estimated the 2014-15 annual report of India’s health ministry, based on studies.
Districts like Sitapur would be the biggest beneficiaries of adolescent health programmes
Over two-thirds of adolescent deaths occur in low and middle income countries. In 2015, about 45% of adolescent deaths occurred in Africa, and 26% in South Asia, where 19% and 30% of the world’s adolescent population lives, according to the World Health Organization.
UP has 185 million children between the ages of 15-19 years, and Sitapur is one of its 25 least developed districts. In Sitapur, in 2015-16, one in three girls was married before they turned 18, in 2010-11, 54 infants died per 1,000 births before they turned one, 54 infants died before 28 days, and 330 of every 100,000 women died during childbirth, according to the latest data available from the National Family Health Survey, 2015-16 and the Annual Health Survey, 2010-11.
The state’s peer education programme chooses two girls and two boys from every village to educate the youth about adolescent sexual health, which would also reduce child marriage and teenage pregnancy. These peer educators go through six days of training by local Accredited Social Health Activists (ASHAs) and Auxiliary Nurse Midwives (ANMs), health workers of India’s national health programme.
Even peer educators can’t access subsidised sanitary napkins
“Most of the problems that girls come to us for have to do with menstrual health and lack of sanitary pads,” said Mausami Bano, as she scanned through the entries in her register, in which she is supposed to keep a record of the problems girls have come to her with. Mausami Bano, a peer educator with the government programme, has completed school and plans to go to college next year.
In 2015-16, in eight states and union territories, not even 50% women used clean methods of dealing with menstrual hygiene, as IndiaSpend reported in June 2017. In UP, only 40% of women used clean methods such as sanitary napkins.
In rural India, 23% of girls listed menstruation as the chief reason for dropping out of school. As many as 28% of them said they do not go to school during their period because they lack clean and affordable protection, according to figures collated by Rutgers, an organisation for sexual and reproductive health and rights.
The lack of access to sanitary pads is felt by every girl in the village, including peer educators Sheetal Raj and Mausami Bano, who have not even once used subsidised sanitary pads, part of the government’s Menstrual Health Programme. The programme subsidises the cost of a six-napkin pack to six rupees under the brand name ‘Freedays’. Usually commercially packed sanitary napkins cost at least Rs 25 for a packet of six napkins. The subsidised napkins should be available at the nearest adolescent friendly health centre clinic (AFHC) in all primary health centres, community health centres and district hospitals.
But for Sitapur, the nearest community health centre with a functioning AFHC clinic is 30 km away from their village, rendering its services inaccessible to most girls. “None of us can travel 30 km to get sanitary pads, so we use cotton cloth instead,” Mausami Bano said.
The primary health centre, which is 8 km from Sameesa village, should have a functioning AFHC with a counsellor, according to RKSK guidelines. In reality, the primary health centre is a dilapidated structure with shattered windows, lying abandoned, as seen on July 29, 2019.
“It has been dysfunctional from the last 5-6 years. I had written a letter to the Chief Medical Officer regarding the state of this hospital but there was no response from the office,” Sonu Kumar, a resident of the neighbouring village of Mehmoodpur, told IndiaSpend.
“Distribution of sanitary pads under the Kishori Shakti Yojana is to be done through junior schools and inter colleges, but Sitapur, since last year, has not been able to procure the tender of sanitary pads due to technical difficulty in accessing the GEM portal (Government e-marketplace). We cannot make our purchase from anywhere else,” said Shiv Kant, Block Coordinator, RKSK, Sitapur.
In Sitapur, in 2014, a sub centre served a population of 8,447 while a PHC served a population of 60,819 and a CHC served a population of 282,372, data from the National Rural Health Mission (NRHM) show, against the standard of 5,000 per sub centre, 30,000 per PHC and 120,000 per CHC, according to Indian Public Health Standards. The district also had 67% fewer specialist doctors, 27% fewer staff nurses and 15% fewer ANMs, according to the NRHM data.
Children unaware about Adolescent Friendly Health Clinics
Since 2014, when the programme began, there have been 7,470 AFHCs established in India, out of which 347 are in UP, according to a reply by India’s health minister’s in the Lok Sabha on July 26, 2019. Of the 21 AFHCs in Sitapur listed by the Population Foundation of India, all except two clinics in Ailiya block were functional. The two clinics had been locked from the past four months since their counsellors were on maternity leave, Shiv Kant told IndiaSpend.
“Very few kids know about adolescent reproductive and sexual health services being provided by AFHC centres in the village,” said Lakshmi Gupta, a counsellor at the AFHC centre in Mishrik block of Sitapur, as she sat in a gloomy ill-lit room with no electricity. “Most of the kids who end up visiting are relatives of ASHAs or for problems such as cough and common cold. There is not enough awareness about the services AFHC centres are meant to provide.”
“I have never heard of AFHC centre and did not know that sanitary pads could be available for cheap,'' said Pushpa Kumari, 14, and a resident of Sameesa village.
Little support to peer educators in RKSK
Mausami Bano and Sheetal Raj are part of the 21.6% of girls in Sitapur who managed to complete 10 years of schooling. RKSK has empowered young women like them, but the programme offers them little support to improve their work or help them solve more complicated problems that might arise.
After they were selected for the RKSK programme, they received a two-day training on adolescent reproductive and sexual health services. After the training, in the past five months, they have met the counsellor only once.
“Frontline workers require greater integration into the RKSK system and orientation on how to reach and engage with adolescents,” said a researcher who works on sexual health issues, but requested anonymity because she worked with the government. Counsellors are recruited with limited years of experience, and it is critical to train them to provide confidential youth friendly services, the researcher explained.
For instance, several times peer educators request Health Education Officers for further guidance or support for issues such as domestic violence, and health workers and counsellors need to be trained to handle such follow-up requests.
Peer educators do not receive any payment or incentive for their work. “This might affect their motivation in continuing the activities after their training,” the researcher said. The researcher suggested financial incentives or a certification which would help them in their career, college admissions, or to get government jobs in the future.
Also, many peer educators, especially girls, find it difficult to reach villages and the community health centre. Providing a bicycle, especially to those female peer educators, may improve their outreach, the researcher suggested.
Not all adolescent issues receive enough attention
There are six themes that RKSK covers: sexual and reproductive health, nutrition, injuries and violence (including gender-based violence), prevention of non-communicable diseases, mental health and substance misuse, according to a 2015 Ministry of Health press release.
But not all themes get equal attention. The programme provides counselling for mental health, but the programme doesn’t have enough experienced professionals to prevent mental health disorders, said Deepak Kumar, a government consultant for RKSK. “Violence, suicide and substance misuse are key areas that still need to be made a priority,” he added.
Low usage of sanitary napkins, but no funds spent on subsidised napkins
In Sitapur, no funds were spent on the procurement of sanitary napkins in the menstrual health scheme from 2016 to 2019, according to a report by Accountability Initiative, a think-tank based in New Delhi.
| Component-Wise RKSK Allocations In Sitapur (Rs lakh), 2016-19 | |||
|---|---|---|---|
| Components | 2016-17 | 2017-18 | 2018-19 |
| Training | 4 | 83 | 85 |
| Printing activity | 0 | 33 | 41 |
| Honorarium | 0 | 3 | 38 |
| Services: facility and community based | 3 | 10 | 8 |
| Procurement of equipment | 4 | 4 | 0 |
| Incentives: ASHA | 0 | 6 | 0 |
| Procurement of drugs and supplies | 0 | 3 | 0 |
| Behavioral change communication | 0 | 0 | 0 |
Source: Accountability Initiative, 2019 (Data shared with IndiaSpend)
Nearly all the funds were spent on procuring weekly iron and folic acid supplements as part of the National Iron Plus Initiative, according to the report. No expenditure was recorded on behavioral change or for creating awareness about the programme, which experts said are the core guiding principle for educating youth about adolescent health. This also explains, in part, why most children do not know about the programme or the clinics.
No allocations were made for ASHA incentives in 2016-17 and 2018-19, “which is surprising given the critical importance of ASHA workers to the implementation of RKSK programmes”, the report noted.
Most funds for RKSK lie unused across UP
In 2015-16, Sitapur had 61.3% women who wanted to delay childbearing but could not access contraception. In 2017-18, RKSK, which also aims to reduce child marriage and teenage pregnancy, was allocated only 1% of the total National Health Mission funding that Sitapur received, falling from 3% in 2016-17, as IndiaSpend reported on July 3, 2019.
Of this money a third was never spent, according to a 2019 analysis of NHM finances by Accountability Initiative.
Source: Accountability Initiative, 2019 (Data shared with IndiaSpend)
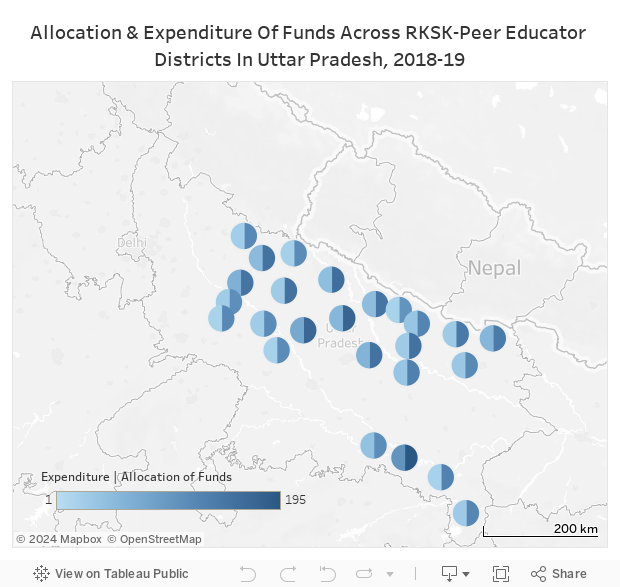
Overall, most districts have spent only part of the funds allocated for the programme. Across UP Sitapur has the second highest allocation of Rs 177 lakh, but spent only Rs 56 lakh--32% of the total funds. It ranked tenth among 25 high priority districts in terms of fund utilisation, according to the Accountability Initiative report. The highest utilisation was in Allahabad with 53% of the funds being utilised.
In 2018-19, 62% of the funds allocated under various heads for training of peer educators and ASHAs were not utilised. Funds utilised for training doubled between 2017-18 and 2018-19, with 38% of the allocated funds being spent, up from 20% in 2017-18. This increase comes mostly from block-level training of peer educators, according to the Accountability Initiative report.
(Ali is a reporter with IndiaSpend.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
