Minister Says Universal Healthcare Is Priority, But Health System Is Under-Staffed

New Delhi: While the Indian government has promised improved and universal healthcare, a new study has pointed out that the country’s healthcare system is under-staffed, does not meet global standards for density and is largely unqualified to meet rural health needs.
“We will make Ayushman Bharat-PMJAY and health and wellness centres into a people’s movement,” union health minister Harsh Vardhan told the media as he took charge of his ministry on June 3, 2019, referring to the prime minister’s national health protection programme, the Pradhan Mantri Jan Arogya Yojana (PMJAY).
Launched in September 2018, PMJAY, the national health protection scheme, offers insurance of up to Rs 5 lakh to 100 million poor households to reduce “catastrophic expenses” and aims to move India towards universal health coverage.
However, it may be difficult to achieve these ambitions given the shortcomings pointed out in a study published in BMJ Open, an open-access medical journal, on May 27, 2019. The density of doctors, nurses and midwives per 10,000 population was 20.6 in 2016, up from 19 in 2011-12--calculated using National Sample Survey Office (NSSO) data--said the study, which also used (registry) data from professional associations such as the Medical Council of India, Indian Association of Physiotherapists, Indian Nursing Council and the Ministry of Health and Family Welfare.
New medical, nursing and paramedical technical education institutes that cropped up over the decade to 2016 were responsible for the increased numbers. “However, this rise is still not enough to meet the minimum standards set by the WHO [World Health Organization] which is 22.8 health workers per 10,000 population,” said Anup Karan, additional professor at the Indian Institute of Public Health, run by the Public Health Foundation of India (PHFI), a Delhi-based advocacy. “About 250,000 health workers are needed to meet this requirement.”
Ensuring that the healthcare system is fully staffed is important because of India’s many health crises, some of which include: 17% of maternal deaths globally; increasing cases of non-communicable diseases, which accounted for 61% of deaths in 2016; and an ongoing struggle to control communicable diseases such as leprosy and malaria. Since most Indians pay out of pocket for health expenses, millions slip into poverty every year because of health catastrophes they cannot afford, as IndiaSpend reported in July 2018.
Healthcare workforce: ‘Most severe crisis’
As we said earlier, according to the WHO norms of 2006, there should be a minimum of 22.8 health workers--including 10 doctors--per 10,000 population: India has 20.6 doctors, nurses and midwives per 10,000 population, and no more than 5.9 allopathic doctors, according to the NSSO.
The Global Health Workforce Alliance, created to address health workforce shortage crisis, and the WHO in 2006 categorised India among 57 countries facing the “most severe crisis” with regard to healthcare human resources.
Ten years later, in 2016, the WHO revised its norms to 44.5 healthcare workers per 10,000, needed to achieve sustainable development goals and universal health coverage. This is almost double of India’s current healthcare workforce numbers.
In 2016, India had a healthcare workforce of 3.8 million, including nurses, mid-wives, doctors, paramedical professionals, health assistants and non-medical personnel, such as administrative and housekeeping staff. Rural India and the eastern states had an even lower density--an average of 17.
However, these estimates do not include 790,000 auxiliary nurse midwives (ANMs), village-level female healthcare workers, who are vital to India’s primary healthcare system. “This is because ANMs are not recognised as nurses according to international standards,” said Karan from the Indian Institute of Public Health.
Initial steps to give ANMs internationally-recognised training and licenses are under way in Telangana, as IndiaSpend reported in February 2019, and could be scaled up as well as replicated in other parts of the country. If ANMs are counted, India has 29 healthcare workers per 10,000, higher than the 2006 WHO norm for human resources for health but still 14.5 workers below its 2016 benchmark.
There was a 1.2 million gap between the number of health workers registered and the data reported by the NSSO. The density of doctors, nurses and midwives was 26.7 using registry data, the gap being attributed to the fact that 20% of these health professionals may be registered but are currently not employed in the healthcare workforce, said the study.
India’s missing women health workers
Much of this shortfall can be attributed to the missing women in India’s healthcare workforce, said the study.
Nearly 19% of those who are “graduate in medicine” and 31% of those with a “diploma or certificate in medicine” are not in the workforce. Among women, 26% graduates in medicine and 46% of those who hold diplomas or certificates in medicine are out of the workforce.
Between men and women, there is an employment difference of more than seven percentage points in employment among graduates and 30 percentage points among those with certificates or diplomas in medicine. With regard to vocational training in health and paramedical services, the proportion of men out of the workforce is greater than women.
“It is noticed that most women in their most productive age face challenges in being in the workforce due to marriage and childcare,” said Karan, and often their families have reservations about their profession.
“Just getting the trained women in the workforce will help India bridge the gap in health worker density to an extent and improve the situation,” he said. Of the 25-35% of women out of the workforce, it would be possible to get at least half of them back through gender-sensitive policies, he said.
Available but not trained
Not all of India’s currently working health professionals are trained: 54% of all healthcare workers, including 25% of allopathic doctors, had “inadequate or no training”, the study said.
The proportion of unqualified workers among the healthcare workforce is similar across the board: pharmacists (62%); health associate professionals, including dieticians, optometrists and physiotherapy assistants (62%); nurses and midwives (58%); and physiotherapist, diagnostician and others (45%).
If only human resources qualified for healthcare are considered, the density comes down to 15.8 per 10,000--seven workers fewer than the 2006 WHO standards. The older standard continues to be used because only developed countries meet the 2016 standards.
The problem of unqualified medical professionals is not unique to India: China, Bangladesh, Uganda and Australia also face this deficit.
However, not allowing these unqualified practitioners to practice would be difficult to enforce in a country like India, said Avani Kapur, director of Accountability Initiative, a public policy think-tank. It may result in many communities having no access to any healthcare at all. “Instead, recognising that we have a large informal network and ensuring training would definitely help since for a large part of India's primary healthcare system, very qualified degrees are not needed for basic outpatient care,” she said.
Conducting training programmes for informal healthcare providers could improve the quality of care, a 2016 study in West Bengal had found, so that more patients would consult them, increasing their income.
The present study suggested that traditional birth attendants, snakebite healers and bone setters, often the first point of contact for rural populations but unqualified as health professionals, could be brought into the “mainstream” by registering them. Also, dais (traditional midwives) could be registered with the government and allowed to deliver babies, while many other workers could be registered as paramedical personnel.
However, there is no clear policy on these workers in India, the paper noted.
The great lag in eastern, central India
With seven healthcare workers per 10,000 population, Jharkhand possesses India’s worst healthcare-workers density, according to the study. Many central and eastern states are similar: 11 (per 10,000) in Assam, 12 in Madhya Pradesh, 20 in Odisha, 23 in Bihar and 25 in the northeastern states. An exception is West Bengal, which has a density higher than the national average with 36 health workers per 10,000.
With 67 health workers, Delhi has the highest density in India, followed by Kerala (66), the union territories (62), Punjab (52) and Haryana (44).
“There is an urgent need to open more medical institutions in the eastern states of India,” said Karan. “Most of these institutions are in the south and the west, which is why doctors from the eastern states end up going there and often don’t return. If more institutes opened in other parts of the country, chances are that the doctors will stay back in their own states.”
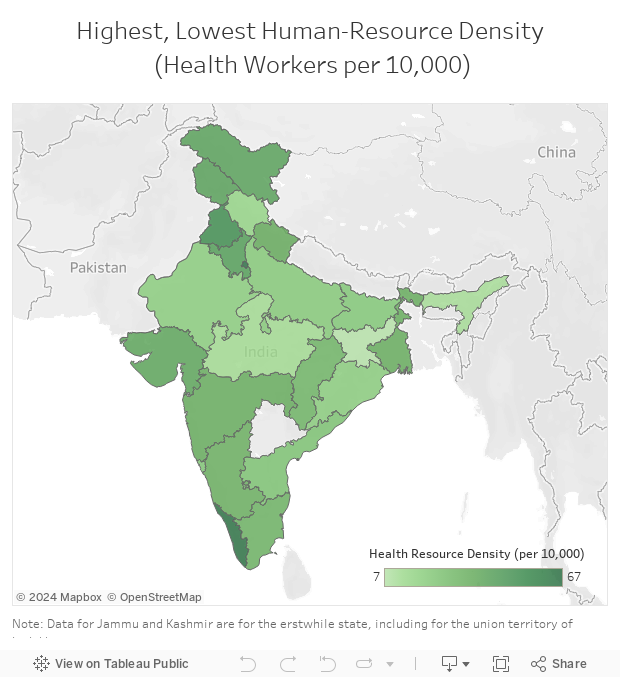
Source: BMJ Open
Most southern Indian states have higher health-worker densities than the all-India average of 29, except Andhra Pradesh with 25 per 10,000, according to the study.
There are rural-urban disparities too. Despite being home to 71% of India’s population, rural India has 36% of its health workers, with densities being especially low for dental practitioners (3.2%) and physiotherapists, diagnosticians and others (14.7%); 34% of doctors and 33% of nurses, respectively, serve in rural India.
Predominantly private
Healthcare in India is driven by private care providers, with 72.4% of the country’s health workforce being engaged in the private sector, according to the study.
Almost all (93.6%) AYUSH practitioners (Ayurvedic, Unani, Siddha and Homeopathy practitioners), 91.7% of dental practitioners, 80.4% of allopathic practitioners and 55.3% of nurses and midwives, practice in the private sector.
Private healthcare in India includes for-profit and nonprofit hospitals and private practitioners: 53% of all health workers are self-employed, and only 6% are employed in large corporate healthcare companies.
This story was first published here on Healthcheck.
(Yadavar is a special correspondent with IndiaSpend.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
