How Karnataka Is Improving Children’s Health By Focusing On Mothers

Ballari, Tumkur and Mysuru: Rekha M, 30, is six months into her second pregnancy and visits the Shankarbande anganwadi (care centre for children in rural areas) in her village for a nutritious meal every day--free of cost. She did not have this provision during her first pregnancy three years ago.
In 1975, when the Indian government launched the Integrated Child Development Services (ICDS), Karnataka was one of the first beneficiaries. The programme tackled maternal malnutrition and morbidity by providing mother and child with supplementary nutrition, immunisation, health check-ups and referral services on nutrition, health education and pre-school education.
Yet, in 2015-16, after four decades of ICDS, Karnataka had the highest maternal mortality ratio (MMR, which measures mothers’ deaths per 100,000 live births) among all the states in southern India--108.
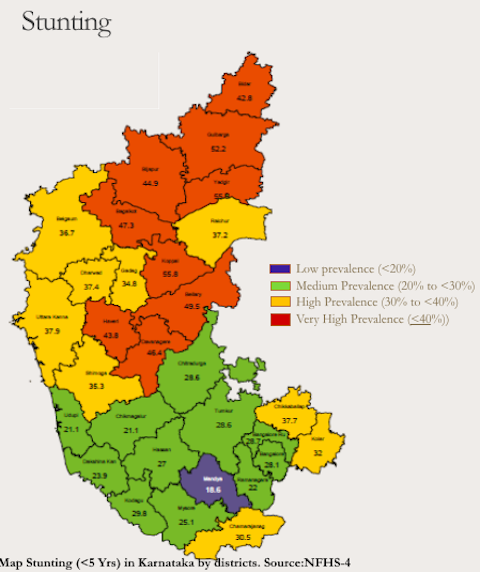
It also had a high rate of stunting (low height for age) and wasting (low weight for height) in children under the age of five--more than a third (36%) of its children were stunted and more than a fourth (26%) were wasted, according to the National Family Health Survey 4, 2015-16 (NFHS-4), the latest available data.
To improve the situation, Karnataka launched the Mathrupoorna scheme in 2017 to fulfil the nutritional needs of pregnant and lactating women.
Similar to ICDS, Mathrupoorna seeks to meet the nutritional needs of pregnant and lactating (till six months post pregnancy) women. The difference being: while ICDS gave the beneficiaries dry rations once a month, Mathrupoorna offers them nourishing hot meals, six times a week. The meals are served at 65,911 anganwadi centres across the state. Women in their ninth month of pregnancy or 45 days post-delivery can have their meals picked up from the anganwadi.
In two years of operation, Mathrupoorna has reached 75% of its target population, according to Karnataka’s women and child development department (WCD), at an annual cost of Rs 645 crore ($91.4 million).
A different approach
It is a hot summer afternoon, and 11 women--eight pregnant and three lactating--are gathered at the anganwadi in Shankarbande village in drought-hit Ballari district. Vandaramma, 62, who goes by one name only, joins the group with an empty steel tiffin box in hand. These women are here for Mathrupoorna.
Anganwadi worker Sulochana and helper Sumitra walk in with large aluminium pots of freshly cooked lunch. Sumitra places a clean steel plate in front of each woman, and Sulochana serves them hot rice, sambhar (south Indian curry consisting of lentils and vegetables) and payasam (a dessert made of rice or vermicelli, and milk). Sumitra informs the women that she has added spinach to the sambhar along with other vegetables to “make it more nutritious”. The women are also given chikki (a jaggery-and-peanut sweetmeat), a glass of hot milk and one boiled egg each. Those who do not like eggs get sprout-salad.
While the women eat, Sulochana packs Vandaramma’s tiffin box with the same meal. It is for her daughter who gave birth 15 days ago and is now resting at home.

Mathrupoorna beneficiaries at the anganwadi in the tribal Maladahadi village in HD Kote taluka (sub-district) of Mysuru district, on the border of the Nagarhole Tiger Reserve. The wholesome meals provided to pregnant and lactating women six times a week take care of 40-45% of their daily calories, protein and calcium intake.
Inspired by similar nutritious meals programmes in Andhra Pradesh and Telangana, Mathrupoorna meals take care of 40-45% of the daily calories, protein and calcium intake of the target group. Mathrupoorna also focuses on the administration of iron and folic acid tablets, deworming, tetanus injection, gestational weight monitoring and counselling of the women.
The ICDS supplementary nutrition programme, which ran earlier, gave pregnant and lactating women and children up to three years of age 1,300 gm of a rice-and-soya mix, 1,200 gm of a wheat-and-soya mix, 900 gm of Bengal gram, 460 gm of green gram and 1 kg jaggery. Though this made up for some of the nutrition gaps, the rations were often shared by other family members. Sometimes the provisions were inadequate or pilfered. Under Mathrupoorna, since women must visit the anganwadi to eat, the aid reaches them in its entirety.
The Mathrupoorna scheme aspires to reach around 1 million (1,023,956) women in the state. Currently, it aids 772,104 pregnant and lactating mothers (including anganwadi workers and helpers who are also beneficiaries), according to the WCD, which implements the programme.
The central and state governments share the cost of the meals, which works out to Rs 21 per meal. While ICDS chips in with Rs 9.50 per meal, the rest is provided by the Karnataka government. “The cost of implementing Mathrupoorna may seem high. However, the cost of inaction is much higher,” said Uma Mahadevan, former principal secretary of WCD.
In February 2017, WCD launched a Mathrupoorna pilot project in four talukas of Karnataka--Manvi in Raichur district, HD Kote in Mysuru, Madhugiri in Tumkur and Jamkhandi in Bagalkot. “The money for the pilot project came from the department’s savings,” said Mahadevan. On October 2, 2017, the state government scaled up the programme to cover the entire state. Mahadevan played a crucial role.
Disturbing facts: stunting and wasting in children
The first 1,000 days of life comprise a unique period of opportunity when the foundations of optimum health, growth and neurodevelopment across the lifespan are established, according to the World Health Organization. “To tackle malnutrition, addressing nutritional needs in the first 1,000 days of life is important,” said Abid Ahmed, a UNICEF consultant assisting Karnataka’s WCD in the implementation of Mathrupoorna.
Stunting in children under five years of age is also worrisome in Karnataka (See graph 1: Nutrition status of under-five children in Karnataka)--36% of its children are stunted and 26% are wasted, according to NFHS-4 data. Between NFHS-3 (2005-06) and NFHS-4 [2015-16], children suffering from wasting and severe wasting have gone up in the state, which is a matter of high concern, said Ahmed. Regional disparity in stunted children is also stark. (See map 1: District-wise ‘stunting’ in under-five children in Karnataka).
“Child stunting in Karnataka is a concern. In 2013, the state government launched the Ksheera Bhagya scheme to provide hot milk (150 ml per child per day) to all the children in anganwadis and government schools thrice a week. This was increased to five times a week in 2017-18, providing valuable calcium, protein and other nutrients,” said Mahadevan. Also, anganwadi children are given eggs twice a week. Eggs provide high-quality protein and choline (essential for the structural development of the body), necessary for young children.
The comfort of a hot meal
“Daily wage labourers like us cannot afford to have milk and eggs,” said Vandaramma at the Shankarbande anganwadi, who belongs to a scheduled caste (traditionally “lower” caste). “Even family members will not feed us if we do not go to work and earn a living.”
Mamtha G is nine months pregnant but continues to visit the anganwadi in Tungoti village in Madhugiri block of drought-hit Tumkur district. Apart from the hot meals, it is also the chance to “step out of the house and interact with other women” that draws her to the anganwadi every day. Meeting other women at the anganwadi also helps deal with postpartum emotional upheavals, she said. Her first child is two-and-a-half years old.
Sudha Ramesh is the mother of a one-and-a-half-month-old baby and is also a regular at the anganwadi. “In our homes, post-childbirth women are offered only rice and watery sambhar; nothing else. At the anganwadi we get vegetables, eggs and hot milk,” she said.
More than 250 km away, similar voices emerge at Maladahadi village in HD Kote taluka of Mysuru district, which lies on the border of the Nagarhole National Park and Tiger Reserve, and is home to the Jenu Kuruba tribe.
Yamuna Ramesh is a native of the village and was registered under the Mathrupoorna scheme from the beginning of her pregnancy. One month back, she gave birth to a healthy baby girl weighing 3 kg. “Traditionally, we eat only two meals a day; rice and sambhar in the morning and ragi [finger millet] balls in the evening,” she said. At the anganwadi, the young mother gets eggs, her favourite, and also leafy vegetables. Anganwadi workers regularly monitor pregnant women like herself for weight gain and mid-upper-arm circumference to check for malnutrition. “We counsel the tribal women to consume lentils and vegetables,” said anganwadi worker Rukmini.

Apart from providing hot meals to pregnant and lactating mothers, Mathrupoorna also focuses on the administration of iron and folic acid tablets, deworming, tetanus injection, gestational weight monitoring and counselling. Here, the anganwadi worker measures a beneficiary’s mid-upper-arm circumference to check for malnutrition.
The challenges
Although Mathrupoorna covers 75% of pregnant and lactating women in Karnataka, there is a wide variation in district-wise coverage. For instance, in Bagalkot district, it is 92%, whereas, in Dakshin Kannada district, it is 27% (See graph 2: District-wise coverage under Mathrupoorna).
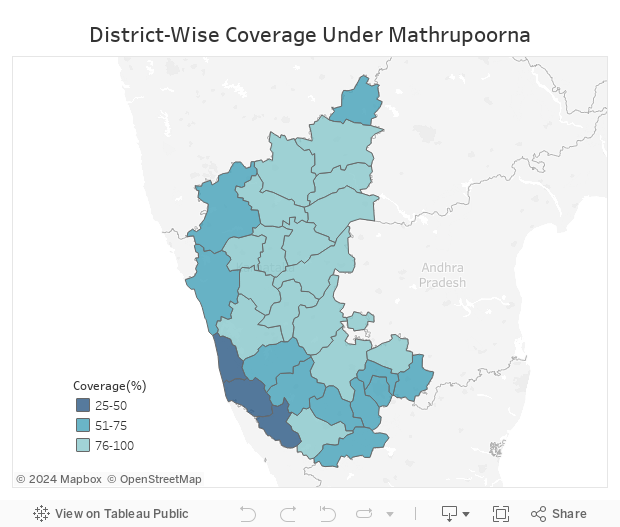
Source: Department of women and child development, Karnataka
“The difference in coverage reflects the divergent needs and socio-economic contexts of various districts,” said Mahadevan. “Karnataka has significant regional differences in poverty levels and human development indicators among its districts.”
Other stumbling blocks include seasonal migration for work.
A large number of women at the anganwadi in Ibrahimpura village, Ballari taluka, where Bashira has worked for the last five years, are daily wage farm labourers. Seven pregnant and four lactating mothers are enrolled under Mathrupoorna here. Child stunting and malnutrition are high in this region of north Karnataka, and mothers are malnourished. “In the summer, the enrolled women, along with their families, migrate to Bengaluru in search of work and often fall out of the anganwadi network,” said Bashira.
To prevent such exigencies, Karnataka government has introduced Thayi cards (mother’s card/a mother and child registration booklet) for pregnant and lactating mothers, which can be used in any district to avail the benefits of Mathrupoorna. However, more often than not, poor women are unable to do so.
There are daily wage earners like eight months pregnant Laxmi, a resident of Shankarbande village, Ballari, who do not get the full benefits of Mathrupoorna. Laxmi leaves home at seven in the morning and returns only around five in the evening. As a farm labourer, she earns Rs 200 a day; men earn Rs 300. “It is not possible for me to leave work mid-way and go to the anganwadi to eat,” she said. She visits the anganwadi on rare occasions when she is not at work.

Social taboos, migration and varying poverty levels are major stumbling blocks for Mathrupoorna. However, one obstacle is overworked and underpaid anganwadi workers. The government programme has increased the burden of anganwadi workers and helpers, according to health sector activists.
Culture and social stigma also prevent women from using the programme. “The local culture does not allow a pregnant woman to step out of the village until she completes five months of pregnancy. So, if the anganwadi is slightly far away, the family does not send a pregnant woman,” informed Bashira. In other areas, sending a pregnant woman to the anganwadi for a meal becomes a “prestige issue”. In Shankarbande village, there are three pregnant women and two lactating mothers who have never visited the anganwadi. “In spite of counselling, their families don’t approve of it,” said Sulochana, an anganwadi worker.
“There is no doubt that decentralised kitchens that serve hot meals and provide basic access to nutrition are welcome. In that sense, Mathrupoorna is a good programme,” said Sylvia Karpagam, a public health doctor and researcher from Bengaluru. “But, there are implementation issues that overburden anganwadi workers and helpers, and exclude some women due to poverty and caste factors.” Anganwadis are primarily child care centres. Mathrupoorna has put an additional burden on anganwadi workers and helpers, Karpagam said. “They spend too much time cooking and serving meals and in the process anganwadi children get neglected. The workers are also underpaid.”
To ease the burden on the workers, the government has provided twin-burner stoves, additional LPG cylinders, pressure cookers and large cooking vessels to anganwadis. “So that the helpers do not spend too much time cooking,” said Mahadevan. The monthly salary of anganwadi workers and helpers has been raised from Rs 4,000 and Rs 3,000 a month to Rs 8,000 and Rs 4,000, respectively. “They also receive Rs 50,000 medical reimbursements,” Mahadevan said.
However, anganwadi workers have demanded better compensation for frontline workers--Rs 18,000 per month for anganwadi workers and Rs 12,000 for helpers.
The success of any such large-scale health programme depends on the frontline staff, Karpagam said. In case of Mathrupoorna, there are 64,800 anganwadi workers and 60,207 anganwadi helpers implementing the programme even in the remotest parts of the state, including inside forest areas. Adequate compensation and regular training of these is vital for further increasing coverage of Mathrupoorna, she added.
Looking Ahead
From speaking to WCD officials, UNICEF consultants, and staff at 15 anganwadis across four districts, here are some steps that could improve Mathrupoorna’s reach and effectiveness:
- Regular training of anganwadi workers and helpers is crucial for pregnant and lactating women’s health monitoring, administering of calcium and folic acid tablets, etc.
- Adequate compensation of the frontline staff, primarily anganwadi workers. This is particularly true of anganwadi workers in villages with less than 300 population, where there is only a mini anganwadi centre staffed by one woman who acts both as an anganwadi worker and helper.
- Digitisation of health records (at present anganwadi workers maintain numerous registers and growth monitoring charts).
(Nidhi Jamwal is environment editor with Gaon Connection.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
