How India Could Fill In The Blanks On Excess Mortality

Chennai: India’s officially recorded deaths have always been problematic, even before the COVID-19 pandemic: just 70% of deaths in India are registered, and only a fifth of these are medically certified, more often than not with the underlying cause of death recorded incorrectly.
Even countries with near-complete registration of deaths in normal times have acknowledged that their officially recorded COVID-19 death tolls might be underestimates, and most of the developed world is now focusing not on directly reported COVID-19 deaths but on excess mortality--the number of deaths above that expected during ‘normal’ times.
The United Kingdom’s Office for National Statistics (ONS) has released weekly excess mortality data, comparing differences between overall mortality for each week this year with the average of the previous five years. By excluding the COVID-19 death toll from this year’s numbers, it found that until May 1, there were 12,900 more “non-COVID-related” deaths in 2020 than in previous years.
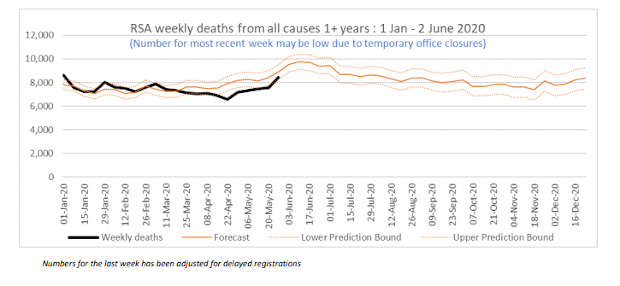
The Financial Times found excess mortality being reported in all but four of the 20 countries that it had compiled data for. Of the countries for which such data are available, South Africa most closely resembles India in income and epidemiological terms, (although it is much richer, with a per capita income nearly twice that of India’s). South Africa does not report excess mortality; on the contrary, it reports reduced overall mortality. Every week since the middle of March 2020, South Africa has reported fewer deaths than the historical trend would have predicted, the South African Medical Research Council (SAMRC) has found. “This is mainly due to the decline in the number of deaths from unnatural causes as well as a slight decrease in the number of natural deaths during the weeks of lockdown,” the SAMRC noted.
South Africa Has Registered Lower All-Cause Mortality This Year
Is it possible to estimate excess mortality in India, given the problems with baseline data?
India’s National Health Mission reports monthly data from over 150,000 health facilities in every district of the country. Data for March 2020 indicated a fall in deaths reported to district hospitals and sub-district hospitals under most categories (data for subsequent months have not been released, though they are usually updated everyday).
All-cause national mortality data are not yet available in India, but data from some cities and states show fewer deaths overall, or lower ‘all-cause mortality’.
In a press conference on May 29, Kerala’s chief minister Pinarayi Vijayan noted that total mortality had fallen in the state until mid-May. "In Kerala, between 1 January and 15 May 2019, 93,717 deaths were recorded,” he said. “This year, during the same period, 73,155 deaths have been recorded. This means the number of deaths this year has been lower by 20,562. COVID was first reported in Kerala at the end of January this year."
As of the end of April, Mumbai had found similarly, as per BMC data shared with IndiaSpend; all-cause mortality had declined as compared to previous months and years.
So can India be certain that it does not have an excess mortality problem? That seems unlikely, some public health experts argue. “I think a real decline in mortality is unlikely, even factoring in fewer accident deaths. More deaths at home, especially for people who tried to seek hospitalisation and were turned away, seems quite widespread,” P. Arokiasamy, demographer and head of Department of Development Studies at the Mumbai-based International Institute of Population Sciences (IIPS), which leads India’s National Family Health Survey operations, said.
Even before COVID-19, it was well established that India’s annual estimates of deaths from disease missed a significant number of deaths, by comparing officially recorded data with estimates using multiple other methods, including verbal autopsies. Official data relying largely on government hospitals estimated 194 deaths from malaria in 2017, while the Global Burden of Disease, which uses multiple sources including verbal autopsies, estimated 50,000 deaths for the same year. Estimates for tuberculosis incidence are 10 times the official numbers, our analysis shows.
So how can India produce excess COVID-related mortality data?
Estimating the extent of excess mortality in India will not be as straightforward as it is in many developed countries, but knowing what Indian mortality statistics already miss will be a good place to start, said Usha Ram, professor and head of the Department of Public Health & Mortality Studies at IIPS.
To begin with, India must quantify the problems with its baseline data. “The baseline data for many states is very poor, so we cannot automatically build on it,” Ram said, “The less developed states have virtually no reliable data on medically certified causes of death, and for smaller states, the sample sizes were so small in the past that their numbers are unusable.”
Then, it will be important to look at diseases that might not appear at first glance to be COVID-related. National Health Mission data point to a significant disruption in health services, including for potentially life-threatening conditions such as cancer and tuberculosis. “These patients will have experienced a severe degeneration in their conditions, including those with chronic kidney disease, diabetes, tuberculosis and heart disease,” said S.P. Kalantri, medical superintendent at the Mahatma Gandhi Institute for Medical Sciences (MGIMS) in Wardha, Maharashtra, which experienced a significant disruption in patients’ access to critical care. The health outcomes of such patients could increase overall mortality.
“The only way we can know if there were excess [deaths attributable to COVID] is if we conduct a sample study post-COVID. Even then, deaths of people who for example could not access dialysis, or from lack of medicines, will be missed,” Arokiasamy said. “Enumerators will need to be trained to ask more probing questions,” Ram said.
India has conducted two national-level household surveys on all-cause mortality in the past, whose architecture it could build on, said Prabhat Jha, founding director of the Centre for Global Health Research in Toronto, and professor of disease control at the University of Toronto. Jha led the Million Death Study in collaboration with the Registrar General of India that produced verbal autopsy-led cause-of-death estimates for 2013 in India. India has not, however, published any verbal autopsy-based data since.
In 2017, the Office of the Registrar General of India tied up with the All India Institute of Medical Sciences to produce more reliable mortality estimates, but no reports have been released yet. “I believe that the 2015 SRS data is now with the Registrar General. I think they should release that immediately, but also prioritise collecting data for the current year,” Jha said, referring to verbal autopsy-based Sample Registration System reports on mortality from India’s Census Commissioner’s Office.
A representative national survey would take time. Until then, better-run cities could be used as a dipstick for urban estimates, Jha suggested. While for less developed and more rural districts updated official data on all-cause mortality can be unreliable, this is less so for the major metros. “In the urban areas, they do have a Register of Deaths that counts the registered deaths. Now the registered deaths don’t give you much detail but reporting those weekly and comparing them--let’s say what happened in each of the weeks of March versus what happened in March 2019 or 2018--can give you a sense to say, well, is there an increase in the overall deaths,” Jha said.
In cities like Mumbai where most deaths take place in hospitals and most crematoria and burial grounds are also run by the civic administration, the Register of Deaths is a much more reliable source of information than say rural Bihar where a majority of deaths take place at home and cremations and burials rarely need permissions, Kaushalendra Kumar, assistant professor at the International Institute for Population Sciences, who focuses on sub-national mortality estimates, said.
“Another strategy is that police coroners in every district could swab all bodies they are conducting autopsies on, and from that you’d get some prevalence in the unrelated dead--people who died from traffic injuries and so on and so forth--to see if they also had COVID,” Jha said.
This is the first part of an ongoing investigation on India's COVID-19 mortality.
(Rukmini S. is an independent journalist based in Chennai.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
