What Child Stunting Numbers Tell Us About North-East Indian States
The states with the highest and lowest percentages of stunted children aged under five among all 22 states and union territories covered in Phase 1 of NFHS-5 are from the North East--Meghalaya and Sikkim, respectively. States with the highest increase and highest decrease in stunting over the past four years are also from the North East--Tripura and Sikkim.

Bengaluru and Delhi: Stunting among children aged below five has increased in four northeastern Indian states, a trend not observed in the region over the last 15 years, according to the fifth round of the National Family Health Survey, 2019-20 (NFHS-5), released in December 2020.
Stunting, or low height for age, is a well-established risk marker for poor development among children. Stunting before the age of two, in particular, has significant economic and educational consequences at the individual, household and community levels. A 1% loss in adult height due to childhood stunting is associated with 1.4% loss in economic productivity, according to a World Bank-supported study. It is estimated that stunted children earn 20% less as adults.
All northeastern states except Arunachal Pradesh were among the 22 states and Union territories covered in Phase 1 of NFHS-5. Meghalaya, Mizoram, Nagaland and Tripura saw an increase in stunting among children, and Assam, Manipur and Sikkim saw a decline. These trends are in contrast with findings of earlier NFHS surveys, where all northeastern states had seen a decline in stunting levels.
Causes for the varying performance in addressing stunting will become clearer when NFHS-5 reports on disaggregated data on access to services and releases indicators for different social groups later this year. Diverse demographics and socio-cultural practices impact child and maternal health within and between states in the northeast, one study shows. Tribal communities in remote areas in the more sparsely populated states have a high prevalence of childhood malnutrition due to limited access to basic amenities including healthcare.
Our analysis of the available data from NFHS-5 also found that the four states which saw an increase in stunting performed poorly on women's well-being indicators, with relatively higher percentages of women having body mass index (BMI) below normal and low levels of education. In contrast, the states with the lowest proportion of stunted children all perform better on women's well-being indicators. Indicators of women's well-being explain the difference between low and high stunting districts in India, studies show.
States' performance on other factors influencing stunting was mixed. For instance, Sikkim, which saw a decline in stunting, also saw declines in infant and young child (IYCF) feeding practices and women's access to healthcare. Meghalaya, which has the highest stunting levels, saw factors like IYCF practices and women's access to healthcare improve. So what explains Sikkim's better performance in reducing stunting? Good governance, experts told us. The role of good governance in the rapid decline in stunting among children has also been highlighted in studies we reviewed.
Meghalaya, Mizoram and Tripura see reversal from improved stunting levels
The states with the highest and lowest stunting levels among all 22 states and union territories in NFHS-5 Phase 1 are from the North East--Meghalaya with 46.5% and Sikkim with 22.3% stunting levels, respectively. Moreover, states with the highest increase and highest decrease in stunting between NFHS-4 and NFHS-5 are also from the North East--Tripura with an increase of 8 percentage points and Sikkim with a decline of 7.3 percentage points.
These trends are in contrast with NFHS-3 and NFHS-4 reports, where all North East states had seen a decline in stunting levels. Meghalaya, Mizoram and Tripura had high declines in stunting levels between NFHS-3 and NFHS-4 (above 11 percentage points), but all three have seen an increase in stunting between NFHS-4 and NFHS-5.
"The trends in stunting in the North East, a long-term issue, are worrying and require examination, even though sample sizes from the region are relatively small. As we attempt to build our understanding of the data, we don't have a real hypothesis [on the causes] at this point in time," Suranjeen Prasad, President of the Guwahati-based governing body of the Public Health Resource Network, told IndiaSpend.
Only maternal nutrition improved in all seven North East states in past four years
Factors influencing stunting, as per the World Health Organization (WHO) framework, are listed in the 'Determinants of stunting during the first 1,000 days of life in Bangladesh' report by health institutes in Bangladesh, published in June 2020. The report categorises causes and contextual (community and societal) factors influencing stunting.
Data on WHO causal factors available in successive NFHS reports include poor maternal nutrition, adolescent pregnancy, low caregiver education, inadequate access to sanitation and water supply, poor IYCF practices, poor nutrient quality and incidence of infection. Data are available for only one contextual factor in NFHS-5--access to healthcare measured by women's access to ante-natal check-ups (ANC) during pregnancy.
Only one factor influencing stunting--maternal nutrition--has seen an improvement in the four years since NFHS-4 in all the seven North East states, measured by the proportion of women with a BMI below normal (see table 2, below).
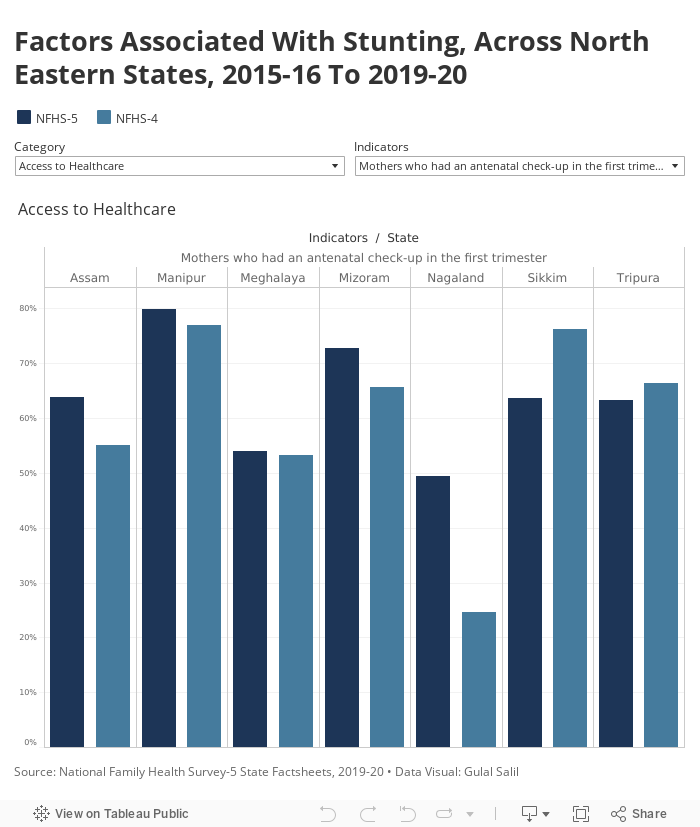
The remaining factors have seen a mixed trend, with corresponding indicators improving in some states and worsening in others. For example, Sikkim, which has seen the highest decline in stunting, saw IYCF practices worsen by 33 percentage points and exclusive breastfeeding decline by 25 percentage points between NFHS-4 and NFHS-5. Access to healthcare also decreased, with women receiving ANCs in the first trimester dipping by 7 percentage points, and those who received at least four ANCs by 16 percentage points. Access to water supply and sanitations also dropped, while the incidence of diarrhoea rose. There was, however, an improvement in caregiver's education and a marginal improvement in children receiving adequate diets.
Similarly, in Meghalaya, which has the highest stunting levels, almost all the factors associated with undernutrition have improved since NFHS-4. Meghalaya has seen an improvement, even if slight, in women's access to healthcare. The percentage of women who had at least four ANCs and level of education of caregivers also slightly increased. Access to water supply and sanitation saw big increases, by nearly 10 and 20 percentage points, respectively. IYCF practices also vastly improved. At the same time, the incidence of diarrhoea slightly declined.
In Manipur, which has seen the second highest decline in stunting levels among the seven states, women's access to healthcare and household's access to drinking water and sanitation has improved by almost 10 percentage points for the former and over 10 percentage points for the latter.
Tripura, which has seen the highest increase in stunting, contrary to its previous trends, saw a worsening of access to healthcare for women, caregiver's education, IYCF practices and prevalence of diarrhoea. For example, the share of women receiving at least four ANCs had declined by 12 percentage points since NFHS-4. The percentage of women with 10 or more years of schooling declined marginally and incidence of diarrhoea increased marginally.
Deterioration of Infant and Young Child Feeding indicators in all seven states
IYCF has been measured by two indicators in NFHS reports--children breastfed within an hour of birth and children exclusively breastfed in the first six months after birth. In addition, we also looked at the proportion of children receiving an 'adequate diet'.
Data show that at least one of these indicators has worsened across all seven states between NFHS-4 and NFHS-5, barring Meghalaya. Assam, Manipur, Mizoram, Sikkim and Tripura saw a decline in the proportion of children breastfed within an hour of birth. Tripura, Sikkim, Nagaland and Manipur saw a decline in the proportion of children exclusively breastfed for the first six months. Nagaland, Mizoram and Assam saw a decrease in the proportion of children receiving adequate diets, an indicator that was already low, averaging at just 16% in all the seven states in NHFS-4.
The trends on IYCF in the North East Region in NFHS-5 reflect the trends observed in these indicators across other states like Goa, Bihar, Gujarat and Karnataka covered in Phase-1.
This is not surprising, Prasad said. "One of the key reasons for us not seeing the kind of improvement we should be in IYCF is because there is no programmatic push from the state or central government on this, as we see in the case of institutional delivery or routine immunisation. Apart from breastfeeding week, there are no reviews or monitoring mechanisms in place to track IYCF indicators and analyse them at the district and state level. In fact, the [central government's] Poshan Abhiyaan, which is focused on behavioural change [for early initiation of breastfeeding, exclusive breastfeeding and timely initiation of complementary feeding] in its current form, is just rhetoric and not delivering for IYCF the way it should be."
North East performs well on indicators of maternal nutrition and education
Analysis shows that the three states with the lowest stunting in the North East all perform better on indicators of women's well-being: BMI and educational attainment. A strong correlation between mothers' BMI and education and childhood stunting levels was found in the Bangladesh study.
Sikkim, Manipur and Mizoram have low proportions of women with BMI below normal, at 5.8%, 5.3% and 7.2% respectively. Nearly half of women in these three North East states have 10 or more years of schooling, at 49.0%, 50% and 48.1%, respectively.
The three states with highest stunting levels among the seven states also perform relatively worse on these two indicators. In Meghalaya, Tripura, and Nagaland, the proportion of women with BMI below normal is 10.8%, 16.2% and 11.1%, respectively. Similarly, the proportion of women with 10 or more years of schooling is 35.1%, 23.2% and 44.4% respectively.
Possible causes for Sikkim's better performance in reducing stunting among children
Sikkim has shown decreased stunting among infants and young children, a 7.3-percentage-point reduction compared to its NFHS-4 levels, despite a worsening of some of the causal factors, as seen above. Sikkim is considered to have the best governance in the North East, followed by Mizoram, said Prasad, which could provide the enabling environment needed to improve stunting rates in Sikkim even without improvements in some of the nutrition determinants in NFHS-5.
The role of good governance in the rapid decline in stunting among children between 2006 to 2012 in Maharashtra is highlighted in a 2014 study by the Institute of Development Studies (IDS). About 39% of infants in Maharashtra state were stunted, according to NFHS-3 (2005-06), but by 2012, around 23.6% were, a decline of nearly 3 percentage points per year, according to the Comprehensive Nutrition Survey in Maharashtra, 2012. This was the fastest decline in the rate of stunting ever recorded, with the next best being Bangladesh. Conditions in Maharashtra were conducive to the rapid declines in stunting on several fronts, including strong economic growth that reduced poverty and moderately good governance with a focus on nutrition, along with well performing underlying (contextual) and immediate (causal) determinants of nutrition, the IDS study found.
Between 2006 and 2016, Sikkim consistently improved the contextual determinants of nutrition, with respect to women's access to education, women's age of marriage and household access to basic amenities, a 2017 study led by the International Food Policy Research Institute (IFPRI) found. Women's nutrition emerged as a key area to prioritise; for instance low women's BMI explained almost a fifth of the difference between high- and low-burden stunting districts in India, showed a 2018 IFPRI study assessing the geographical burden of stunting in India. The latter study also suggests that other variables on women's well-being like education, age at marriage and education explain close to half the difference between low and high stunting districts in India. Sikkim performs best after Mizoram on women with 10 or more years of schooling and women's literacy in the North East, NFHS-5 findings reveal.
While findings and interventions in the North East cannot be compared and translated to most other states in India, "data from the North East needs to be analysed carefully as there is much that the states within the region can learn from each other and there is a need to document the best practices," Prasad suggests.
"In the past, we generalised that improving trends in nutrition in North East India could be due to their local practices, the strong local government laws and the ability to maintain food sovereignty because of these laws. The recent NFHS-5 findings should spur us to gain an in-depth understanding of the disparities between the states and help us understand the determinants at play in nutrition in the region," said Prasad.
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
