Health Crisis Needs Money—But That Isn’t Enough

India bears 21% of the global disease burden, losing at least 6% of gross domestic product (GDP) to premature death and preventable illness.
Every indicator is grim. About 90% of treatments for childhood diarrhoea and pneumonia–the leading causes of death among Indian children–are wrong and 56 out of every 1,000 kids under the age of five died in 2012.
It seems to be obvious that India should be spending a lot more on healthcare than its current spend of 1.3% of gross domestic product (GDP) and the proposed Rs 1.93 lakh crore ($31 billion) over the 12th Plan (2012-2017).
Yet, that may not be so obvious either.
Many studies have pointed to the fact that health outcomes are not necessarily related to increased spending, leading to this comment in The Hindu that the 2015 Draft National Health Policy was putting a “band-aid on a corpse”.
This study, for instance, noted that seven of 17 states could do better, not by spending more money, but by being more efficient.
Poorer Bangladesh and Haiti spend more of its GDP than India with 3.6% and 6.4%, respectively.
But in many poor, large Indian states, medical-personnel shortages are rife and vast areas have no healthcare on offer, so while efficiency of spending must improve, in these cases, more spending is important.
The Bharatiya Janata Party-led government, set to announce its first full-fledged budget on February 28, promised in its manifesto to increase spending on health to 3% of GDP.
Let us look at the budget outlay for the Department of Health and Family Welfare over the past three years.
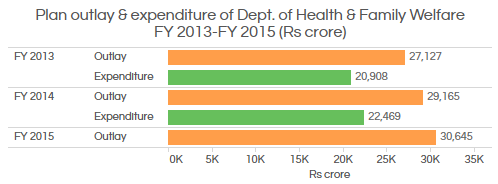
Source: Ministry of Health and Family Welfare
The approved outlay in plan expenditure for the department has increased from Rs 27,127 crore in 2012-13 to Rs 30,645 crore in 2014-15, an increase of 13%. The actual expenditure has increased 7.5% from Rs 20,908 crore (77% utilisation of approved outlay) in 2012-13 to Rs 22,469 crore (77% utilisation) in 2013-14.
Health outcomes across the country have improved over the past few years. The infant mortality rate (IMR) and maternal mortality ratio (MMR) have fallen. However, there are wide disparities between states.
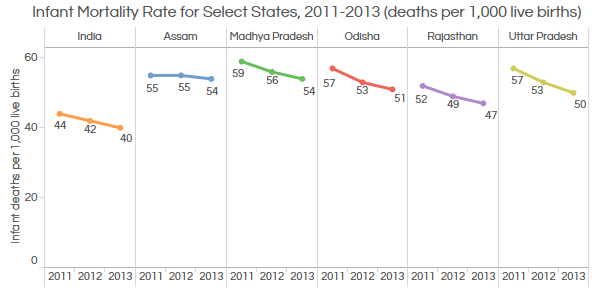
Source: Lok Sabha
The overall infant mortality rate (IMR) has declined from 44 deaths per 1,000 live births in 2011 to 40 in 2013.
Assam and Madhya Pradesh had the highest IMR at 54 deaths per 1,000 live births, the same as Liberia and Ghana.
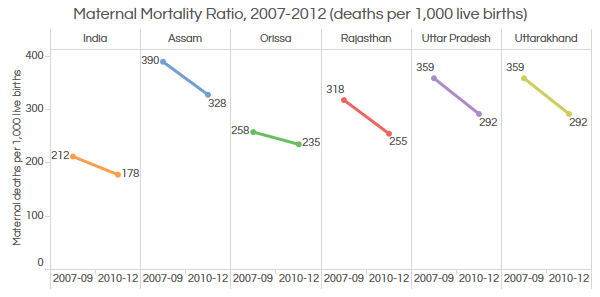
Source: Lok Sabha
The all-India maternal mortality ratio has declined from 212 per 1,000 live births to 178 in 2012. Assam has the highest MMR with 328 per 1,000 live births followed by Uttar Pradesh with 292 deaths per 1,000 live births in 2012, higher than Rwanda with 320 and Equatorial Guinea with 290.
One of the main reasons for the disparity in outcomes is the unequal distribution of healthcare infrastructure.
State-owned primary health centres (PHCs) that operate in rural areas are essentially single-physician clinics usually with facilities for minor surgeries. Community health centres (CHC) work as the referral centre for four PHCs, covering a population of 80,000 to 120,000.
As many as 8,760 PHCs (nearly 36.4% of 24,448 PHCs nationwide) now offer 24x7 services across the country, according to the Ministry of Health and Family Welfare. However, there is a shortage of these health centres with a 24% shortfall in the number of PHCs across India and 33% in the number of CHCs.
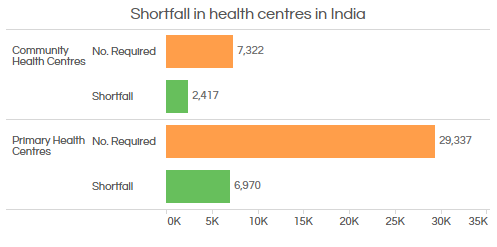
Source: Ministry of Health and Family Welfare
Let us now look at the availability of doctors at these centres across India.
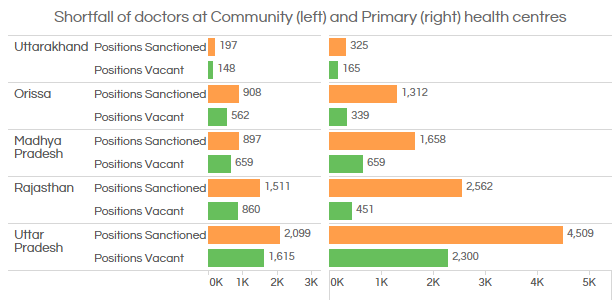
Source: Ministry of Health and Family Welfare
All over India, there is a 25% shortfall of doctors in PHCs and 67% in CHCs.
Uttarakhand, Uttar Pradesh and Madhya Pradesh are short of doctors by 51% and 40%, respectively. The vacancy at CHCs is even steeper in these states at 77%, 75% and 73%, respectively.
Infrastructure spending, which meets expenses for construction of PHCs/CHCs and salaries for doctors, nurses as well as medical staff, has actually declined over the past two years from 23% of the budget to 15% in 2014-15.
So, the challenges would be to increase spending on health infrastructure, reduce the gap between rural and urban areas when it comes to health outcomes, focus on curbing the spread of communicable diseases and, above all, show greater efficiency in health spending. We will wait for some answers on February 28.
_____________________________________________________________
“Liked this story? Indiaspend.org is a non-profit, and we depend on readers like you to drive our public-interest journalism efforts. Donate Rs 500; Rs 1,000, Rs 2,000.”
