27 Regional Hubs, 300 Hospitals, Yet Patients Journey To 1 Mumbai Cancer Centre

1 million are diagnosed with cancer every year; 680,000 of them die. India’s cancer burden to rise 70% by 2035.
Mumbai: Carrying thin plastic bags full of medical reports, about 30 cancer patients queue up outside Pankaj Chaturvedi’s office on the second floor of the Homi Bhabha Wing of the 76-year-old Tata Memorial Hospital in the central suburb of Parel. Some are too weak to stand. So, they sit down, sometimes on the floor. As a receptionist tries to maintain order in the overcrowded lobby, the volume of patients and attendants–mostly relatives–swells.

Pankaj Chaturvedi, head and neck cancer specialist, examining a patient in his cabin at Tata Memorial Hospital, Mumbai.
Chaturvedi is a specialist in head-and-neck cancer, the most common kind in India, accounting for a quarter of all registrations at Tata Memorial, which is run by the central government’s Department of Atomic Energy. The wing from which he works was built to accommodate “private” patients, those who pay the actual costs of medical care, but he examines everyone; 60% of patients fall in what is called the “general category”, which allows them to get free or highly subsidised treatment, depending on whether they live below the poverty line or just above it.
With India’s cancer-care facilities limited to a handful of major cities, the poorest patients make long, desperate journeys to Tata Memorial, either for a proper diagnosis or medical care, as the first and second part of this series explained. Today, in the concluding part, we explore how Tata Memorial Hospital is coping with a flood of cancer patients and study the Indian government’s cancer-care plans for the country’s poorest patients.
It takes up to eight hours to see a doctor in the general out-patient department (OPD), and here at Chaturvedi’s office the wait is less but still up to three to four hours, according to patients.
“We do not operate and treat less complex cases, we send them back,” Chaturvedi told IndiaSpend in between examinations. “I may have sent 30% of our patients back to their native place.” There are facilities back there that can treat these cases, but that treatment is provided after an endorsement from Tata Memorial, he said.

India has one oncologist for 1,500 patients (in the US, it is one per 100) and they are concentrated in about eight metropolitan cities, which why cancer patients have to travel extensively for treatment.
India has one oncologist for 1,500 patients (in the US, it is one per 100 and in the UK one per 400), and they are concentrated in about eight metropolitan cities, according to 2015 study by the consulting firm Ernst and Young. Mortality rates are higher than the West because of late diagnosis and treatment and the prevalence of cancer is likely to rise 70% over the next 18 years, as Indians age, become more obese, smoke, drink more liquor, breathe polluted air and drink polluted water.
While the government has changed priorities of the 50-year-old national cancer programme from tertiary treatment to early diagnoses, some experts question the implementation and financing of the changeover. Non-communicable diseases, such as cancer, now account for 60% of all deaths in India, but received less than 3% of the national health budget in 2017-18, as we explain later. The result is that cancer awareness and prevention is low.
Chaturvedi attributes the particularly high burden of head-and-neck cancer to the Indian affinity for cigarettes, beedis, and chewing tobacco. India had 810,000 tobacco users, and 28.6% of adults above the age of 15 used tobacco in any form, according to Global Adults Tobacco Survey (GATS) 2016-17. Life for head and neck cancer patients is severely affected because the cancer affects their ability to speak and eat.

The scene at the head-and-neck cancer department at the Tata Memorial Hospital, which sees 300 patients in the out patient department and conducts seven surgeries every day.
Every day, the head-and-neck cancer department sees 300 patients in the OPD and conducts seven surgeries in almost an “assembly line” set-up, each of which typically lasts three to four hours. Most patients do not respond well to radiation and chemotherapy and surgery is usually required. “Very few institutes offer surgery which should be the first line of treatment for oral, cervical, breast cancer the top cancers in India and which occur in the poorest and instead offer only radiotherapy,” said Chaturvedi. “So patients end up coming here.”
Waiting time for surgery can stretch to one month in an overstretched hospital
Tata Memorial is the workplace of choice for some of India’s best oncologists; it has the country’s best equipment and is well-funded. It is also overstretched, according to its administrators, treating about 65,000 new patients and 450,000 follow-up patients every year, much over capacity.
Most of the hospital’s other 11 departments appear as pressured as the head-and-neck cancer department, and the 11 OPDs are always full. Patients assigned for surgery have to wait up to one month for their turn during which their disease progresses and adds their cost of living.
These pressures are manifest in the form of patients who live on the pavement outside the hospital. Each of 51 street-dwelling patients IndiaSpend surveyed had spent an average of three months, either waiting for diagnosis or getting medical care. Most had made long journeys, often cross-country, with 41% from Bihar and 17% from Uttar Pradesh; eight of 10 were daily wage labourers; 44% were jobless when cancer struck, and 92% had a grade VII education or less.
What most had in common was that they had ended up on footpaths outside Tata Memorial after seeking treatment in other government or private hospitals, although some came here when physicians or doctors urged them to.
All district hospitals offer cancer care, so why the flood in Parel?
In an ideal scenario, tertiary care centres such as Tata Memorial Hospital should not see this flood of patients, since all district hospitals in India offer some sort of chemotherapy and surgery, and 14,379 government medical colleges nationwide have radiation facilities. India has a national cancer-control programme, with 27 regional cancer centres and 300 other multispecialty hospitals treating cancer. The National Cancer Institute at Jhajjar, Haryana, with a budget of Rs 2,035 crore (in 2017), has the largest budget of any cancer-care centre in India.
The reason they flock to Tata Memorial is apparently reputation and desperation, our conversations with patients revealed. It is also a reflection of the current “horizontal” healthcare delivery system--with its primary health centres and others above it--Anil D’Cruz, director of Tata Memorial, told IndiaSpend.
“What we really need is a diagonal healthcare delivery system to look at diseases individually along with (normal) health delivery,” said D’Cruz. For instance, cancer often has similar symptoms as other diseases--such as cardiovascular afflictions or diabetes--and diagnoses should be made earlier at secondary health care centres.
Only cases that require specialised treatment should, ideally, come to tertiary care centres such as Tata Memorial, as Chaturvedi, the head-and-neck cancer specialist, said, explaining why his department returned a third of cases to regional cancer centres.
Yet, despite a national cancer programme that is now half a century old, Tata Memorial is a hospital of both last and first resort.
From tertiary treatment to primary diagnosis, cancer care is trying to change
The national cancer-control programme may be 50 years old, but 68% of Indian cancer patients die before five years of diagnosis. In contrast, 60% of cancer patients survive beyond five years of diagnosis in North America and Europe.
The disparity in survival is more pronounced in rural areas which is why even though the incidence of cancer in rural areas is half that of urban areas, mortality rates are similar in both urban and rural areas, suggesting that patients in rural areas are at higher risk of dying.
India does not have enough oncologists, and those available are concentrated in about eight cities, as we said. When the national cancer programme was launched in 1975, it focussed on equipping tertiary cancer institutes with infrastructure. Since 1984, the focus changed to prevention of cancer and early detection, moving later to developing district cancer-care centres.
A national cancer registry was established in 1984 by the Indian Council of Medical Research to record cancer incidence and patterns, using data from 21 population-based registries--which cull data on all new cases of cancer occurring in a well-defined population--and six hospital-based registries which record cancer cases in particular hospitals.
Cancer is part of the national programme for the prevention and control of cancer, diabetes, cardiovascular diseases and stroke (NPCDCS), launched in 2010 and being implemented under National Health Mission (NHM) with district-level interventions in 36 states and union territories.
For a long time, cancer care was a top-down effort, focussing on treatment and tertiary care, ignoring screening, early detection or prevention in primary care. That focus appears to be changing, as the government tries to do more than it has before.
Cancer has been made a health priority, but the money must follow
The national cancer programme now includes health promotion activities, opportunistic screening and, as the effort to control noncommunicable diseases (NCDs), includes oral, cervical and breast cancers.
By June 2017, 419 District NCD Clinics and 2,116 CHC NCD Clinics were set up. With operating guidelines drafted and published, cancer screenings may soon begin across India’s districts.
Not everyone is convinced of the approach.
“India has a NRHM [national rural health mission] hangover,” said Subhojit Dey, part of the Global Burden of Disease project, and co-chairman of the Cancer Interest Group at Delhi’s Public Health Foundation of India (PHFI), an advocacy. Maternal and child health and communicable diseases have been India’s priority until now. The fact that cancer was added to the NPCDCS in 2009, a year after guidelines were issued, indicates the priority given to cancer, said Dey.
Although non-communicable diseases were responsible for 60% of deaths in India in 2014, they received no more than 2.65% (Rs 1,255 crore) of the 2017-18 health budget (Rs 47,352 crore); 44% of the budget has gone to the NRHM.
Some experts argue that clubbing cancer with other non-communicable diseases may not be a good idea because cancer treatment is far more complex and expensive and screening for cancer can require more training than screening for diabetes or hypertension.
“There are more than two dozen types of cancers, which need specialists at the primary treatment stage,” said Preet Dhillon, associate professor and epidemiologist at the PHFI’s Centre for Chronic Conditions and Injuries. “There is also a different stigma attached to cancer, which requires a different degree of sensitisation.”
However, Dhillon said, screening for cancers as part of the national programme is a “good beginning”, indicating priority to cancer. “There are still many questions [about cancer policy], but without doubt, we have come farther than ever before,” she said.
The Indian government is also planning an additional 20 state cancer institutes and 50 tertiary care cancer centres. The National Cancer Institute at Jhajjar, Haryana, will be open by August 2018, and will be India’s best-funded public cancer-centre with a budget of Rs 2,035 crore, said G K Rath, head of radiotherapy at All India Institute of Medical Sciences and the doctor appointed to head the institute. “It will conduct translational research--practical application of research findings--on cancers that affect Indians,” said Rath.
Most cancer deaths occur because a majority of Indian patients are at an advanced stage of the disease when they seek care. With better screening and awareness and robust cancer treatment at government institutes, these deaths can be prevented, said Rath.
A national cancer grid holds promise, allows oncologists to collaborate
Cancer care in India does not follow standard protocols, so a national cancer grid (NCG), established in 2012, holds promise. The Grid is supposed to link cancer centres--private and public--nationwide, so they follow uniform standards of care based on evidence-based management guidelines and do collaborative research.
Currently 110 centres, 40% of them private, are part of the NCG, treating 600,000 patients between them--60% of India’s cancer burden. Apart from setting guidelines, these institutes also expertise and do collaborative research together.
Over the last six months, at a predetermined time, 120 to 150 cancer experts from across India, log on to the NCG’s platform on what they call a “virtual tumour board”—a video conference where they discuss complex cases.
This should also make cancer treatment more affordable. “A large amount of money (that a patient pays) is coming to a tertiary care centre, and patients spend money in staying for a few days and travelling back (and forth),” said C S Pramesh, head of thoracic surgery at Tata Memorial Hospital and coordinator of NCG. “This can be prevented by providing the same level of care at the patient’s doorsteps.”
But this is, yet, in the future. For now, cancer care is driving patients deeper into poverty.
High cost, catastrophic expenditure drives cancer patients to poverty
In the first part of this series, we told you the story of army aspirant Arvind Kumar--an eye eaten away by cancer--who had seen six doctors in five cities and travelled 2,200 km before landing up on the footpath outside Tata Memorial.
Kumar’s story illustrates the failures of the current healthcare system, especially the government-run system.
It is known that 7% of Indian households are pushed into poverty due to catastrophic health expenditure, an economic term for a family’s health expenses when they exceed by 40% the family’s ability to pay.
Despite the fact that 25% of Indians are covered either by state or private insurance, having health insurance does not reduce either out-of-pocket expenditure--money paid by households from savings for healthcare--or impoverishment due to a health crisis, according to a 2016 analysis by Brookings India, a think tank.
Out-of-pocket expenditure accounts for more than 67% of healthcare costs in India and includes out-patient expenses not covered by health-insurance programmes.
Currently, most cancer patients in India, as we said, die within five years of diagnosis, with poorer patients, as research shows, less likely to survive the disease than richer ones. After treatment, there is no social security for patients to fall back on.
Those who survive may not be able to work after treatment, and their families continue to spend more money on their medicines. In the second part of this series, we calculated a Rs 55,000 loss in income, for the patient and his or her attendant, usually a relative.
Although it is more expensive and spurs catastrophic expenditure, the private sector accounts for 78% of all outpatient visits and 60% of in-patient stays for cancer.
“The reason why patients seek care at private institutes despite the high cost is the quality,” said the PHFI’s Dey. “Quality of care in private institutions is much better than government ones. It is a tough call to make--to look for affordability or for quality.”
This rush to the private sector is made worse because the government’s programmes to finance healthcare languish--either because few patients know about them or procedures to use them are complex.
Under-utilised: Government healthcare-finance schemes
The government provides a variety of financial assistance to patients living the below poverty line (BPL) for life-threatening diseases:
-
Rashtriya Arogya Nidhi (RAN or National Health Fund) allows BPL patients to seek treatment at any of super-specialty hospitals upto Rs 200,000.
-
Health Minister’s Cancer Patient Fund (HMCPF) uses a corpus Rs 100 crore as fixed deposit; the interest is used to provide financial assistance to BPL patients.
-
State Illness Assistance Fund (SIAF), where 50% of the funds are provided equally by the state and the Centre; selected BPL patients can get up to Rs 150,000.
-
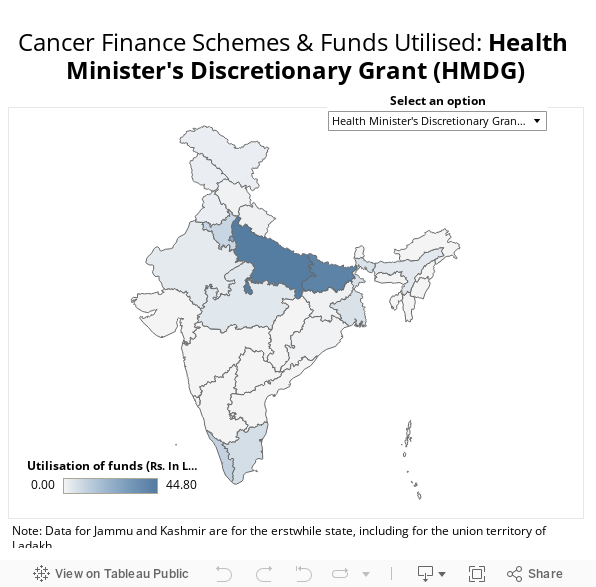
Health Minister’s Discretionary Grant (HMDG), which allows patients earning less than Rs 125,000 annually to get assistance of a similar amount.
Source: Lok Sabha
Other than Puducherry, no state has used the SIAF. In 2016-17, the HMCPF was not used by Karnataka, Gujarat, Odisha, Andhra Pradesh and eight other states. Bihar and Uttar Pradesh used 45% of the RAN funds, while states such as Maharashtra, Karnataka, Chhattisgarh used none.
As the government’s current programmes falter, and the cancer-care network awaits expansion, the poorest patients--it appears--will continue to make their long journeys to the pavement outside Tata Memorial.
Series concluded. You can read the first part here and the second part here.
(Yadavar is a principal correspondent at IndiaSpend.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
__________________________________________________________________
“Liked this story? Indiaspend.org is a non-profit, and we depend on readers like you to drive our public-interest journalism efforts. Donate Rs 500; Rs 1,000, Rs 2,000.”
